Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart defect characterized by four abnormalities: pulmonary stenosis, ventricular septal defect, overriding aorta, and right ventricular hypertrophy. It results in deoxygenated blood being shunted to the body instead of the lungs. Clinical manifestations include cyanosis, clubbing, and decreased activity tolerance. Diagnosis involves echocardiogram, chest X-ray, and cardiac catheterization. Management includes supplemental oxygen, medications during spells, and complete surgical repair typically before age 2 to close defects and reduce obstructions. Complications can include hypoxia, heart failure, and arrhythmias if left untreated.
2. INTRODUCTION
• Tetralogy of Fallot (TOF), first
described in 1888 and named after
Louis Arthur Fallot. Tetralogy of
fallot - the most common congenital
heart disorders.
• TOF is classified as a cyanotic heart
disorder because TOF results in an
inadequate flow of blood to the
lungs for oxygenation.
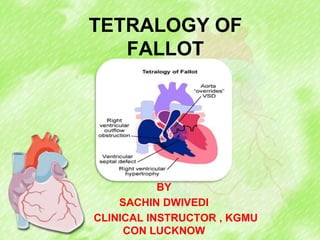
3. DEFINITION
Tetralogy of fallot is a congenital heart defect
which is characterised by the combinations of four
defects :
• Pulmonary stenosis (right ventricular
outflow tract obstruction).
• Ventricular Septal Defect.
• Overriding or dextroposition of the
aorta
• Right ventricular hypertrophy.
4.
5. Incidence
• Tetralogy of Fallot (TOF) represents approximately
7%-10% of congenital heart diseases (CHDs), and
it is the most common cyanotic CHD, with 0.23-0.63
cases per 1,000 births.
6. ETIOLOGY
• Unknown
• Genetic factor:TBX1 Gene
• Methylene tetrahydrofolate reductase
(MTHFR) gene polymorphism
• Maternal rubella during pregnancy
• Poor prenatal nutrition
• Maternal alcohol use
• Maternal age older than 40 years
• Maternal phenylketonuria and diabetes.
7. PATHOPHYSIOLOGY
Obstruction of blood flow from the right ventricle
to the PA results in deoxygenated blood being
shunted across the VSD and into the aorta
Degree of cyanosis depends on the size of the
VSD and the degree of RVOTO
Due to structural defects, there is right to left
shunt causing cyanosis
8. Minimal RVOTO results in a pink or acyanotic TOF
The right ventricle becomes hypertrophied as a
result of the increased gradient across the RVOT
RVOTO can occur at pulmonary valve stenosis,
infundibular stenosis, or supravalvular stenosis.
9. CLINICAL MANIFESTATIONS
• Cyanosis
• Tet spells
• Squatting position
• Slow weight gain and mental
slowness.
• Difficulty with feeding and
failure to thrive.
• Clubbing
• Polycythemia
• Decreased activity tolerance
10. DIAGNOSTIC EVALUATION
• Auscultation
o Harsh systolic ejection
murmur heard best at
the upper left sternal
border.
o During a hypercyanotic
spell the murmur
disappears.
11. DIAGNOSTIC EVALUATION
• Chest X-ray
o Boot shaped because of
pulmonary stenosis with
an upturned apex
resulting from Right
Ventricular Hypertrophy
12. DIAGNOSTIC EVALUATION
• Hematologic studies
o Haemoglobin and hematocrit values
are usually elevated in proportion to
the degree of cyanosis.
o Prolonged cyanosis causes reactive
polycythemia that increases the
oxygen carrying capacity.
13. Coagulation studies
• There is diminished coagulation
factors and diminished total
fibrinogen, which are associated
with prolonged prothrombin and
coagulation times.
17. MANAGEMENT
• Supplemental oxygen - to compensate
for restricted pulmonary blood flow
• Analgesics- Most analgesic agents
have sedating properties, which are
beneficial for patients who are having
hypercyanotic episodes
18. MANAGEMENT
• Morphine sulfate, 0.1-0.2 mg/kg
intramuscularly (IM) or subcutaneously
(SC), may decrease systemic venous
return as well as producing a sedative
effect that provides comfort and
diminishes anxiety for the patient
19. MANAGEMENT
• Alpha-adrenergic Agonists
• Phenylephrine, 0.02 mg/kg IV, is
used to increase SVR. This drug
produces vasoconstriction of
arterioles, thereby increasing
peripheral venous return.
• Improve myocardial contractility
• Increased heart rate and CO.
20. MANAGEMENT
• IV propranolol (Inderal) may be
administered, which relaxes the
infundibular muscle spasm causing
RVOTO.
21. Management of "tet" spells
• Infant can be placed in a
knee-to-chest position if
possible. This provides a
calming effect, reduces
systemic venous return, and
increases Systemic Vascular
Resistance (SVR).
• Morphine sulfate
• Alpha-agonist phenylephrine
22. SURGICAL MANAGEMENT
• The timing of complete surgical repair is
dependent on numerous variables,
including symptoms and any associated
lesions (Eg. Multiple VSD).
• The trend is to perform a complete
surgical procedure before the age of 1
year and preferably by the age of 2 years.
Studies have shown, however, that
surgery is preferably done at or about 12
months of age.
24. SURGICAL MANAGEMENT
CORRECTIVE
• Closure of the
ventricular septal defect
utilizing a patch.
• The infundibular
obstruction can be
surgically resected to
reduce the amount of
restriction