
Download to read offline



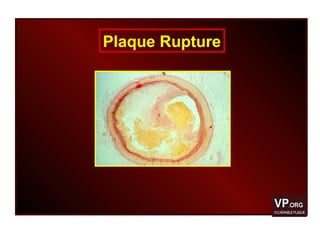



This editorial discusses positive (expansive) remodeling as a potential surrogate marker for plaque inflammation and vulnerability. The editorial summarizes several studies that found associations between expansive remodeling and histological markers of vulnerable plaques as well as unstable clinical presentations. One such study found that plaques with expansive remodeling had larger lipid cores and more macrophages compared to plaques with constrictive remodeling in patients who died from coronary artery disease. While expansive remodeling prevents luminal narrowing long-term, it may destabilize plaques and increase risk of rupture in the short-term. Further research is needed to understand the predictive value of arterial remodeling patterns and identify ways to induce beneficial expansive remodeling without increasing plaque vulnerability.






































































































