EDSP 360
Lesson Component
Criterion
Points Possible
Points Earned
Subject and Grade Level
Subject and grade level are identified.
1
Topic
Topic is identified.
1
Standards
State and national standards are written out. Standards relate to the lesson.
2
Objective
Objective is written in the proper condition, performance, criteria format. Performance is written in a measureable term.
5
Diversity/
Differentiated Instruction
Class description is briefly described including students with disabilities. Teacher candidate describes what portions of the lesson is differentiated for each subgroup. Five differentiations are noted, each based on a disability represented.
15
Materials
Complete list of materials are given.
1
Technology Connection
Specific technology connection is identified, including web address and/or name of computer program to be used.
1
Character Education
Principle
Scripture and reference are provided. Description of how the principle is taught in the lesson.
5
Procedures:
Set
Introduces the lesson and provides a creative way to engage students in the lesson.
5
Procedures:
Instruction
Detailed description of how the teacher candidate plans to teach the skill. How the skill will be modeled is fully explained. All components of objective are addressed.
15
Procedures:
Guided Practice
A practice activity where the teacher guides the class is provided. All components of objective are addressed.
7.5
Procedures:
Independent Practice
A practice activity where the teacher allows students to work independently is provided. All components of objective are addressed.
7.5
Closure
Closure recaps the main point of the lesson.
4
Evaluation
A tool to assess the objective is provided. Expected mastery level is stated. Matches the objective.
5
Total Points
75
Instructor Comments:
Project 3: Lesson Plan Grading Rubric
The Journal of Emergency Medicine, Vol. 52, No. 1, pp. 8–15, 2017
� 2016 Elsevier Inc. All rights reserved.
0736-4679/$ - see front matter
http://dx.doi.org/10.1016/j.jemermed.2016.07.108
RECEIVED: 26 Se
ACCEPTED: 26 Ju
Brief
Reports
COMPARISON OF METAL AND PLASTIC DISPOSABLE LARYNGOSCOPE BLADE
WITH REUSABLE MACINTOSH BLADE IN DIFFICULT AND INHALATION INJURY
AIRWAY SCENARIO: A MANIKIN STUDY
Andreas Moritz, MD, Sebastian Heinrich, MD, Andrea Irouschek, MD, Torsten Birkholz, MD,
Johannes Prottengeier, MD, and Joachim Schmidt, MD
Department of Anesthesia, University Hospital of Erlangen, Erlangen, Germany
Reprint Address: Andreas Moritz, MD, Department of Anesthesia, University Hospital of Erlangen, Krankenhausstr. 12, 91054 Erlangen,
Germany
, Abstract—Background: Single-use plastic blades
(SUPB) and single-use metal blades (SUMB) for direct
laryngoscopy and tracheal intubation have not yet been
compared with reusable metal blades (RUMB) in difficult
airway scenarios. Objective: The purpose of our manikin
study was to compare the effectiveness of these different
laryngoscope blades in a difficult airway ...
1. EDSP 360
Lesson Component
Criterion
Points Possible
Points Earned
Subject and Grade Level
Subject and grade level are identified.
1
Topic
Topic is identified.
1
Standards
State and national standards are written out. Standards relate to
the lesson.
2
Objective
Objective is written in the proper condition, performance,
criteria format. Performance is written in a measureable term.
5
Diversity/
Differentiated Instruction
Class description is briefly described including students with
disabilities. Teacher candidate describes what portions of the
lesson is differentiated for each subgroup. Five differentiations
are noted, each based on a disability represented.
15
Materials
2. Complete list of materials are given.
1
Technology Connection
Specific technology connection is identified, including web
address and/or name of computer program to be used.
1
Character Education
Principle
Scripture and reference are provided. Description of how the
principle is taught in the lesson.
5
Procedures:
Set
Introduces the lesson and provides a creative way to engage
students in the lesson.
5
Procedures:
Instruction
Detailed description of how the teacher candidate plans to teach
the skill. How the skill will be modeled is fully explained. All
components of objective are addressed.
15
Procedures:
Guided Practice
A practice activity where the teacher guides the class is
provided. All components of objective are addressed.
7.5
3. Procedures:
Independent Practice
A practice activity where the teacher allows students to work
independently is provided. All components of objective are
addressed.
7.5
Closure
Closure recaps the main point of the lesson.
4
Evaluation
A tool to assess the objective is provided. Expected mastery
level is stated. Matches the objective.
5
Total Points
75
Instructor Comments:
Project 3: Lesson Plan Grading Rubric
The Journal of Emergency Medicine, Vol. 52, No. 1, pp. 8–15,
2017
� 2016 Elsevier Inc. All rights reserved.
0736-4679/$ - see front matter
http://dx.doi.org/10.1016/j.jemermed.2016.07.108
RECEIVED: 26 Se
ACCEPTED: 26 Ju
Brief
4. Reports
COMPARISON OF METAL AND PLASTIC DISPOSABLE
LARYNGOSCOPE BLADE
WITH REUSABLE MACINTOSH BLADE IN DIFFICULT AND
INHALATION INJURY
AIRWAY SCENARIO: A MANIKIN STUDY
Andreas Moritz, MD, Sebastian Heinrich, MD, Andrea
Irouschek, MD, Torsten Birkholz, MD,
Johannes Prottengeier, MD, and Joachim Schmidt, MD
Department of Anesthesia, University Hospital of Erlangen,
Erlangen, Germany
Reprint Address: Andreas Moritz, MD, Department of
Anesthesia, University Hospital of Erlangen, Krankenhausstr.
12, 91054 Erlangen,
Germany
, Abstract—Background: Single-use plastic blades
(SUPB) and single-use metal blades (SUMB) for direct
laryngoscopy and tracheal intubation have not yet been
compared with reusable metal blades (RUMB) in difficult
airway scenarios. Objective: The purpose of our manikin
study was to compare the effectiveness of these different
laryngoscope blades in a difficult airway scenario, as well
as in a difficult airway scenario with simulated severe inha-
lation injury. Methods: Thirty anesthetists performed
tracheal intubation (TI) with each of the three laryngoscope
blades in the two scenario manikins. Results: In the inhala-
tion injury scenario, SUPB were associated with prolonged
intubation times when compared with the metal blades. In
the inhalation injury scenario, both metal laryngoscope
blades provided a quicker, easier, and safer TI. In the diffi-
cult airway scenario, intubation times were significantly
prolonged in the SUPB group in comparison to the RUMB
5. group, but there were no significant differences between
the SUPB and the SUMB. In this scenario, the RUMB
demonstrated the shortest intubation times and seems to
be the most effective device. Conclusions: Generally, results
are in line with previous studies showing significant disad-
vantages of SUPB in both manikin scenarios. Therefore,
metal blades might be beneficial, especially in the airway
management of patients with inhalation injury. � 2016
Elsevier Inc. All rights reserved.
, Keywords—difficult airway; inhalation trauma; laryn-
goscope blade; manikin study
ptember 2015; FINAL SUBMISSION RECEIVED: 13
ly 2016
8
INTRODUCTION
Complications arising from difficult or failed tracheal
intubation (TI) remain a leading cause of anesthesia-
associated morbidity and mortality (1). There is a higher
incidence of difficult and failed laryngoscopy and high
laryngeal grade views when patients were managed in a
prehospital setting (2). Inhalation injury has become the
most frequent cause of death in acute phase of burn pa-
tients, and can be associated with a difficult airway
caused by acute upper airway obstruction and the pres-
ence of soot in the pharynx (3–5). Therefore, the
equipment for TI in prehospital emergency care should
meet the requirements for difficult intubation
conditions, even in the presence of inhalation trauma.
However, in prehospital emergency care, single-use
plastic laryngoscope blades are often provided for TI
for hygienic reasons. Dos Santos et al. described in their
retrospective prehospital cohort study, conducted during
two 3-year periods at a single university-based
6. emergency medical services system, a plastic disposable
blade intubation rate of > 40% (6). Several clinical studies
suggested that the use of plastic disposable laryngoscope
blades in prehospital emergency care decreases the
success rate of TI when compared with reusable metal
laryngoscope blades, which might have a distinct impact
to difficult airway scenarios (6,7). However, disposable
May 2016;
Figure 2. Erlanger Inhalation Injury Manikin, a modified Laer-
dal Medical AS manikin. The difficult airway is simulated by
cervical immobilization applying a cervical collar. The phar-
ynx is pigmented with activated carbon.
Effectiveness of Laryngoscope Blades in a Difficult Airway
Scenario 9
metal blades have not been compared with reusable metal
and disposable plastic blades in difficult airway scenarios
in a single study. The purpose of this study was to
compare the effectiveness of a single-use plastic blade
(SUPB), a single-use metal blade (SUMB), and a reusable
metal blade (RUMB) in a simulated difficult airway
scenario caused by a rigid cervical collar, as well as in
a simulated inhalation injury airway scenario that
combines a difficult airway and a limited view caused
by a sooted pharynx.
MATERIALS AND METHODS
Thirty anesthetists with a median clinical experience of
3.5 years (interquartile range 2�6 years) voluntary
participated in this randomized crossover trial. Data
were anonymized and information on the performance
of individual participants was not made available to
7. anybody outside the research team. We notified local
ethics committee of the University Erlangen-Nürnberg
about the study. The ethics committee waived a formal
submission for approval.
Each anesthetist performed TI with a SUMB (dispos-
able Macintosh cold light laryngoscope blade, size 3, P.J.
Dahlhausen & Co. GmbH, Cologne, Germany), a SUPB
(disposable laryngoscope blade Macintosh, size 3,
Intersurgical GmbH, Sankt Augustin, Germany), and a
RUMB (reusable X-LITEMacintosh laryngoscope blade,
size 3, Wirutec Rüsch Medical Vertriebs GmbH,
Sulzbach, Germany) (Figure 1) in a difficult airway
scenario manikin (Laerdal Medical AS, Stavanger,
Norway), as well as an inhalation injury airway scenario
manikin (Erlanger Inhalation Injury Manikin, a modified
Laerdal Medical AS manikin) (Figure 2).
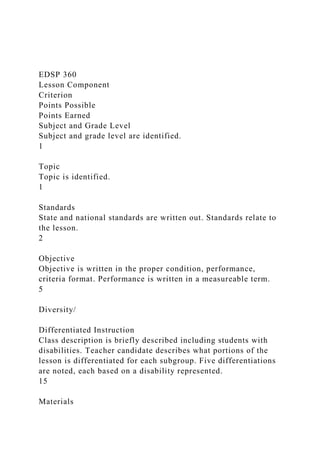
Figure 1. The three different laryngoscope blades used in
this study. From top to bottom: single-use metal blade
(disposable Macintosh cold light laryngoscope blade, size
3, P.J. Dahlhausen & Co. GmbH, Cologne, Germany), single-
use plastic blade (disposable laryngoscope bladeMacintosh,
size 3, Intersurgical GmbH, Sankt Augustin, Germany), and
the reusable metal blade (reusable X-LITE Macintosh laryn-
goscope blade, size 3, Wirutec Rüsch Medical Vertriebs
GmbH, Sulzbach, Germany).
To simulate an inhalation injury, the pharynx of the
Erlanger Inhalation Injury Manikin was pigmented with
activated carbon (Figure 3). The neck of both manikins
was fixed in a neutral position by a rigid cervical collar
and thus the distance between the free edge of the upper
and lower incisors (interdental distance) was limited.
These conditions turned it into a difficult intubation
model (8).
Figure 3. Oropharynx of the Erlanger Inhalation Injury
Manikin. To simulate an inhalation injury, the pharynx is pig-
8. mented with activated carbon.
10 A. Moritz et al.
The order in which the manikins were tested was
randomized by opening two sealed opaque envelopes
containing the names of the manikins. The sequence of
laryngoscope blade use was also randomized for each
scenario by using three sealed opaque envelopes
containing the names of the laryngoscope blades.
Thermal injury to supraglottic structures results in
edema and can rapidly lead to upper airway obstruction
(9). Therefore, all intubations were performed with a
6.0 mm cuffed endotracheal tube ([ETT]; Super
Safetyclear endotracheal tube, internal diameter
6.0 mm; Wirutec Rüsch Medical Vertriebs GmbH,
Sulzbach, Germany) and a laryngoscope handle with
LED illumination (Heine Standard F.O., Heine Optotech-
nik GmbH & Co. KG, Herrsching, Germany). Before
each intubation attempt, a reusable endotracheal tube
introducer was inserted into the ETT. The cuff was
lubricated with a silicone spray and the cuff was inflated
and deflated with a 10-mL syringe.
In order to compare the different laryngoscope blades,
the intubation process was divided into three different
time episodes:
1. The duration of a successful intubation attempt was
defined as the time from insertion of the blade
between the teeth until the ETT was connected to
a self-inflating resuscitation bag and the presence
of lung inflation was confirmed (‘‘time to
ventilate’’).
9. 2. The time to visualization of the glottis (‘‘time to
vocal cords’’) was defined as the time from
insertion of the blade between the teeth until the
glottis was visualized.
3. The time to TI (‘‘time to intubate’’) was defined as
the time from insertion of the blade between the
teeth until the ETT was expected to be correctly
positioned.
The primary endpoint was the ‘‘time to ventilate’’.
Esophageal intubations, attempts requiring > 120 s, and
more than two attempts, were recorded as failed intuba-
tion attempts. All time measurements were made by the
same person by direct observation with a stopwatch to
avoid interobserver error.
We recorded the rate of successful intubation, the
number of intubation attempts, and the laryngeal view
according to the Cormack�Lehane score. The number
of optimization maneuvers (readjustment of the head
position, application of external laryngeal pressure, and
the need for assistance by a second person) and the
number of audible dental click sounds indicating dental
damage were recorded as 0, 1, and $2 times during the
TI attempt. After completing the procedure, each
anesthetist was asked to score the view, the rigidity of
the blade, the intubation effort, the difficulty of use of
each investigated device, and the overall impression
using a numeric rating scale (0 to 100 mm, from
excellent/very easy to poor/very difficult). After each
scenario, the participants were asked to indicate their
preferred laryngoscope blade.
Statistical comparisons were only made within the
10. two airway scenarios. Data for the success of TI
attempts were analyzed using the c2 test. Data for the
number of intubation attempts, time to vocal cords,
time to intubate, time to ventilate, number of
optimization maneuvers, number of dental clicks,
Cormack�Lehane score, view, rigidity of the blade,
intubation effort, difficulty of use of each device, and
overall impression were analyzed using the Krus-
kal�Wallis rank test with Bonferroni correction. All
analyses were performed by Statistica 6 software
(StatSoft GmbH, Hamburg, Germany). Statistical
significance was accepted at p < 0.05. Continuous data
are presented as mean (standard deviation), ordinal
data were presented as medians (interquartile range),
and categorical data were presented as percentages.
The sample size estimation was based on time to venti-
late duration. After a pilot study period, we estimated that
the time required for the successful intubation attempt
would be 19 s for the RUMB, the gold standard for this
study, with a standard deviation of 5 s, in the difficult
airway scenario. We considered an absolute change of
25% in the duration of TI as a clinically significant
change, in numbers, a reduction to 14 s or an increase
to 24 s. With an a error of 0.05 and b error of 0.2, for
an experimental design incorporating three equal-sized
groups, we estimated that at least 22 participants would
be required.
RESULTS
Participant Characteristics
Thirty anesthetists participated in the study (4
pre-registration house officers, 18 senior house officers,
7 specialist registrars and 1 consultant; 17 males and 13
females; mean age of 31 years).
11. Scenario 1: Difficult Airway
All anesthetists intubated the trachea successfully with all
three different laryngoscope blades. There was no
difference in the number of required TI attempts between
the different laryngoscope blades. Each anesthetist
intubated the trachea with a single attempt. There were
no significant differences between SUPB and SUMB in
the recorded intubation times. The time to visualize the
glottis (time to vocal cords) (p = 0.020) and the time to
ventilate (p = 0.044) were significantly shorter with the
Effectiveness of Laryngoscope Blades in a Difficult Airway
Scenario 11
RUMB compared with the SUPB. There were no
differences for the severity of dental compression, the
Cormack�Lehane score and the number of optimization
maneuvers, with only one anesthetist requiring more than
one optimization maneuver with the SUPB. The RUMB
required less effort during TI (p = 0.004) and was judged
as easier to use than the SUPB (p = 0.002). Although the
SUMB was considered to be more stable compared with
the SUPB (p < 0.001), the RUMB was considered to be
even more stable than the SUMB (p = 0.005) and the
SUPB (p < 0.001). Regarding the overall impression
of the devices, the participants rated the RUMB
best. Forty-three percent (95% confidence interval [CI]
26–62.3%) preferred the RUMB, followed by the
SUMB (10%) (95% CI 2.6–27.7%). Forty-three percent
(95% CI 26–62.3%) of the anesthetists would use the
RUMB as well as the SUMB in the normal difficult
airway scenario (Table 1).
Table 1. Tracheal Intubation Data for the Different
12. Laryngoscope
Intubation Data SUMB
Overall success rate, n (%) [95% CI] 30 (100) [85.9–100]
No. of intubation attempts, n (%) [95% CI]
1 30 (100) [85.9–100]
2 0 (0) [0–14.1]
3 0 (0) [0–14.1]
Median (IQR) 1 (1–1)
Severity of dental compression, n (%) [95% CI]
0 22 (73.3) [53.8–87]
1 5 (16.7) [6.3–35.5]
$2 3 (10) [2.6–27.7]
Median (IQR) 0 (0–1)
No. of optimization maneuvers, n (%) [95% CI]
0 27 (90) [72.3–97.4]
1 3 (10) [2.6–27.7]
$2 0 (0) [0–14.1]
Median (IQR) 0 (0–0)
Time to vocal cords, s, median (IQR) 5.9 (4.5–8.4)
Time to intubate, s, median (IQR) 12.1 (9.6–14.7)
Time to ventilate, s, median (IQR) 20.2 (16.6–24.3)
View, cm, median (IQR) 2 (1–3)
Rigidity, cm, median (IQR) 2 (1�3){
Intubation effort, cm, median (IQR) 3.6 (2–5.8)
Overall impression, cm, median (IQR) 2 (1�3)k
Difficulty of use, cm, median (IQR) 2.1 (2–4)
Cormack-Lehane score, median (IQR) 2 (1–2)
Preferred laryngoscope blade, n (%) [95% CI]
RUMB 13 (43.3) [26–62.3]
13. SUMB 3 (10) [2.6–27.7]
SUMB and RUMB 13 (43.3) [26–62.3]
No difference 1 (3.3) [0.2–19.1]
CI = confidence interval; IQR = interquartile range; RUMB =
reusable m
plastic blade.
Data are reported as median (IQR) or as n (%) [95% CI,
including conti
* p < 0.001, plastic blade vs. metal blade.
† p < 0.05, plastic blade vs. Macintosh laryngoscope blade.
‡ p < 0.01, plastic blade vs. Macintosh laryngoscope blade.
§ p < 0.001, plastic blade vs. Macintosh laryngoscope blade.
k p < 0.05, metal blade vs. Macintosh laryngoscope blade.
{ p < 0.01, metal blade vs. Macintosh laryngoscope blade.
Scenario 2: Inhalation Injury Airway
The rate of successful TI and the number of TI attempts
were not significantly different between the groups. How-
ever, the failure rate was 3.3% (95% CI 0.2–19.1%) with
the RUMB, as one attempt was requiring > 120 s, and 0%
(95% CI 0–14.1%) with the SUMB and 10% (95% CI
2.6–27.7%) with the SUPB, respectively. Using the
SUMB or the RUMB, the participants only required
one attempt to intubate the trachea in the prescribed
time. With the SUPB, 20% (95% CI 8.4–39.1%) of the
anesthetists required more than one TI attempt. The
time to visualize the glottis (time to vocal cords)
(p < 0.001; SUPB vs. RUMB) (p = 0.004; SUPB vs.
SUMB), the time to TI (time to intubate) (p < 0.001;
SUPB vs. RUMB) (p = 0.033; SUPB vs. SUMB), and
the time to ventilate (p < 0.001; SUPB vs. RUMB)
(p = 0.045; SUPB vs. SUMB) were significantly shorter
Blades in the Difficult Airway Scenario
SUPB RUMB
15. with the SUMB and the RUMB, when compared with the
SUPB. There were no significant differences in the
severity of dental compression and the number of
optimization maneuvers. However, using the SUPB,
20% (95% CI 8.4–39.1%) of the anesthetists required
two or more optimization maneuvers and caused two or
more dental clicks. The RUMB demonstrated advantages
over the SUPB, including a better view of the glottis
(p = 0.002) and a lower Cormack�Lehane score
(p = 0.012). Both metal laryngoscope blades (RUMB
and SUMB) required less effort during TI (p < 0.001;
SUPB vs. RUMB) (p = 0.015; SUPB vs. SUMB) and
were considered by the anesthetists to be more stable
(p < 0.001) and easier to use (p < 0.001; SUPB vs.
RUMB) (p = 0.034; SUPB vs. SUMB) when
compared with the SUPB. Regarding the overall
impression of the devices, the participants rated the
RUMB and the SUMB higher than the SUPB
(p < 0.001). There was no significant difference between
Table 2. Tracheal Intubation Data for the Different
Laryngoscope
Intubation Data SUMB
Overall success rate, n (%) [95% CI] 30 (100) [85.9–100]
No. of intubation attempts, n (%) [95% CI]
1 30 (100) [85.9–100]
2 0 (0) [0–14.1]
3 0 (0) [0–14.1]
Median (IQR) 1 (1–1)
Severity of dental compression, n (%) [95% CI]
0 27 (90) [72.3–97.4]
1 1 (3.3) [0.2–19.1]
$2 2 (6.7) [1.2–23.5]
16. Median (IQR) 0 (0–0)
No. of optimization maneuvers, n (%) [95% CI]
0 24 (80) [60.9–91.6]
1 5 (16.7) [6.3–35.5]
$2 1 (3.3) [0.2–19.1]
Median (IQR) 0 (0–0)
Time to vocal cords, s, median (IQR) 11.7 (8.2–17.5)
Time to intubate, s, median (IQR) 21.2 (14–31.4)
Time to ventilate, s, median (IQR) 29.6 (23.4–46.4)
View, cm, median (IQR) 4 (3–6)
Rigidity, cm, median (IQR) 2 (1–3.9)
Intubation effort, cm, median (IQR) 4.5 (4–7.9)
Overall impression, cm, median (IQR) 2.6 (1.2–4)
Difficulty of use, cm, median (IQR) 5 (3–7)
Cormack�Lehane score, median (IQR) 2 (2–2)
Preferred laryngoscope blade, n (%) [95% CI]
RUMB 15 (50) [31.7–68.3]
SUMB 12 (40) [23.2–59.3]
SUMB and RUMB 2 (6.7) [1.2–23.5]
SUPB and RUMB 1 (3.3) [0.2–19.1]
CI = confidence interval; IQR = interquartile range; RUMB =
reusable m
plastic blade.
Data are reported as median (IQR) or as n (%) [95% CI,
including conti
* p < 0.05, plastic vs. metal blade.
† p < 0.01, plastic vs. metal blade.
‡ p < 0.001, plastic vs. metal blade.
§ p < 0.01, plastic vs. Macintosh laryngoscope blade.
k p < 0.001, plastic vs. Macintosh laryngoscope blade.
the two metal laryngoscope blades. Fifty percent (95%CI
31.7–68.3%) of the participants preferred the RUMB,
17. followed by the SUMB with 40% (95% CI 23.2–
59.3%) in the inhalation injury airway scenario (Table 2).
DISCUSSION
Difficult or failed TI is not uncommon in a prehospital
emergency setting. Airway management in patients
with symptomatic inhalation injury poses significant
challenges because of acute upper airway obstruction
and decreased visibility due to soot in the oropharynx
(3,10). Prior studies have demonstrated that in
prehospital emergency care, the use of a plastic
disposable laryngoscope blade decreases the success
rate of TI, and that metal disposable blades are superior
to single-use plastic blades at first attempt and the overall
number of attempts to intubate (6,7). Evans and
colleagues demonstrated that the use of plastic blades
Blades in the Inhalation Injury Airway Scenario
SUPB RUMB
27 (90) [72.3–97.4] 29 (96.7) [81–99.8]
24 (80) [60.9–91.6] 30 (100) [85.9–100]
5 (16.7) [6.3–35.5] 0 (0) [0–14.1]
1 (3.3) [0.2–19.1] 0 (0) [0–14.1]
1 (1–1) 1 (1–1)
24 (80) [60.9–91.6] 26 (86.7) [68.4–95.6]
0 (0) [0–14.1] 1 (3.3) [0.2–19.1]
6 (20) [8.4–39.1] 3 (10) [2.6–27.7]
0 (0–0) 0 (0–0)
18 (60) [40.8–76.8] 25 (83.3) [64.6–93.7]
6 (20) [8.4–39.1] 4 (13.3) [4.4–31.6]
6 (20) [8.4–39.1] 1 (3.3) [0.2–19.1]
18. 0 (0–1) 0 (0–0)
20.2 (13.5–31.8)†k 8.9 (7–12.8)
32.9 (23–45.1)*k 17.4 (12.9–23.7)
42 (32.7–56.4)*k 27.2 (22–35.3)
5.6 (4�8)§ 3 (1.1–5)
7.1 (5–8.5)‡k 0.6 (0–2)
7.8 (6.1–8.9)*k 3.9 (3–7)
8 (4.9–9)‡k 1.5 (1–2.1)
8.8 (5.1–8)*k 3.5 (2.9–5.9)
2 (2�3)§ 2 (1–2)
etal blade; SUMB = single-use metal blade; SUPB = single-use
nuity correction].
Effectiveness of Laryngoscope Blades in a Difficult Airway
Scenario 13
results in both greater peak force and duration of
laryngoscopy (11). However, in prehospital emergency
care, single-use plastic laryngoscope blades are often
provided for TI, as there is no need for hygienic
reprocessing. In our manikin study, we aimed to evaluate
the performance of different laryngoscope blades when
used by anesthetists in a difficult airway, as well as an
inhalation injury airway scenario.
In the difficult airway scenario, no significant
differences in the recorded intubation times were
observed between the two disposable laryngoscope
blades. The results may be related to the simulated
difficult, but not inhalation injury modified airway.
Without light-absorbing activated carbon, the anesthetists
19. can identify landmarks of the anatomy and may be able to
perform successful intubation with less peak force and a
slightly more flexible laryngoscope blade, such as the
SUPB. In contrast, without being able to identify
landmarks of the anatomy in the inhalation injury
scenario, the likelihood of a faster TI may be higher
with a less flexible laryngoscope blade. Scholz et al.
demonstrated that anesthetists can see the larynx at very
low light levels in a manikin, but that for a difficult
intubation scenario, a higher light level is necessary
(12). In our study, the participants rated the overall
impression of SUMB higher than SUPB in the difficult
airway scenario. The RUMB demonstrated further
advantages over the SUPB, including significantly
shorter time to vocal cords and time to ventilate. This
can be due to the properties of rigidity of the RUMB. In
the difficult airway scenario, the RUMB was considered
by the anesthetists to be even more stable when compared
with the two disposable laryngoscope blades. Thus, the
maximum stability could explain the faster intubation
times even in the difficult, but not inhalation injury
modified, airway. Buléon et al. demonstrated, in a
randomized single-center study with 1863 adults
requiring general anesthesia, that glottic exposure was
significantly better in the metallic reusable group
compared with the plastic single-use group (13). No
significant differences in the recorded intubation times
were observed between the RUMB and the SUMB.
This is consistent with the findings of Evans et al. (11).
In the inhalation injury scenario, the SUPB was
associated with prolonged intubation times when
compared with the SUMB and the RUMB. In addition,
our study showed that the SUPB had more dental clicks
than the metal blades (Table 2). Although, Itoman et al.
demonstrated, based on a dental fracture model study,
20. that plastic laryngoscope blades have a lower potential
for dental fracture when compared with metal laryngo-
scope blades in routine intubations, these results may
be related to the difficult anatomical orientation in the
inhalation injury scenario (14). With the SUPB, a greater
peak force is required to visualize the glottis (11).
Without landmarks of the anatomy, the participants might
have used the more flexible SUPB with more leverage
force to obtain a direct view of the glottis. Thus, a greater
number of dental clicks with the SUPB could result in a
higher number of dental fractures. The prolonged
intubation times in the inhalation injury scenario could
be explained by the different properties of rigidity of
metal and plastic laryngoscope blades. Goodwin et al.
demonstrated that disposable metal blades are less
flexible in the primary axis than single-use plastic blades
(15). The ratings of the participants confirm these
findings. Both metal laryngoscope blades required less
effort during TI and were considered by the anesthetists
to be more stable and easier to use when compared with
the SUPB. In patients with symptomatic inhalation injury
and acute upper-airway obstruction, the emergency TI
with a less flexible metal laryngoscope blade may be
easier because of the better alignment of the oral,
pharyngeal, and tracheal axes. This could partially
explain why most of the participants preferred the metal
laryngoscope blades in the inhalation injury manikin
scenario. Although, the RUMB demonstrated further
advantages over the SUPB, there was no significant
difference between the disposable and the reusable metal
laryngoscope blades. Similar findings have been found
in previous studies. Jabre et al. demonstrated that for
out-of-hospital patients requiring emergency TI, the
first-pass intubation success with SUMB was noninferior
to first-pass success with RUMB (16).
21. Limitations
This study has some limitations. First, this study is a
manikin and not a clinical study. However, the simulation
of intubation scenarios in anatomically correct manikins
has been described to be a reliable surrogate for the
clinical context (17). Second, the potential for bias exists,
as the study could not be blinded to either the participants
or the assessors. Third, the anesthetists were aware that
their actions were being timed, which could lead to an
altered performance, as a result of the Hawthorne effect
(18). Fourth, we compared only one disposable metal
and one plastic laryngoscope blade with one standard
RUMB. There are various other types of disposable metal
and plastic blades, as well as reusable blades available,
and their properties for direct laryngoscopy in the
difficult airway caused by inhalation injury might be
different and should be investigated. Fifth, because of
the potential upper airway obstruction caused by
oropharyngeal edema in patients with inhalation injury,
all intubations were performed with a 6.0 mm cuffed
ETT. The results might have been different using another
size or brand of ETT. Sixth, certain measurements used in
14 A. Moritz et al.
this study, such as grading the difficulty of use, have a
subjective nature. However, there was good agreement
between the collected subjective data and the objective
measurements, such as TI times. Seventh, this study
was carried out by anesthetists, experienced in the use
of disposable and reusable blades. Thus, results may
differ in the hands of less-experienced users. Finally,
though the SUPB was associated with statistically
significant prolonged intubation times, the clinical impact
22. of this time difference remains uncertain. Further
comparative studies in a clinical setting are necessary to
confirm our findings.
CONCLUSIONS
In the inhalation injury scenario both, the reusable and the
single use metal laryngoscope blades provide a quicker,
easier, and safer TI compared with the SUPB when
used by anesthetists. In the difficult airway scenario, the
RUMB demonstrated the shortest intubation times and
seems to be the most effective device. We therefore
hypothesize that metal laryngoscope blades might be
beneficial, especially in the airway management of burn
patients.
REFERENCES
1. Peterson GN, Domino KB, Caplan RA, Posner KL, Lee LA,
Cheney FW. Management of the difficult airway: a closed
claims
analysis. Anesthesiology 2005;103:33–9.
2. Timmermann A, Eich C, Russo SG, et al. Prehospital airway
man-
agement: a prospective evaluation of anaesthesia trained
emergency
physicians. Resuscitation 2006;70:179–85.
3. Mlcak RP, Suman OE, Herndon DN. Respiratory management
of
inhalation injury. Burns 2007;33:2–13.
4. Haponik EF, Meyers DA, Munster AM, et al. Acute upper
airway
injury in burn patients. Serial changes of flow-volume curves
and
23. nasopharyngoscopy. Am Rev Respir Dis 1987;135:360–6.
5. Moylan JA, Adib K, Birnbaum M. Fiberoptic bronchoscopy
following thermal injury. Surg Gynecol Obstet 1975;140:541–3.
6. Dos Santos FD, Schnakofsky R, Cascio A, Liu J, Merlin MA.
Disposable stainless steel vs plastic laryngoscope blades among
paramedics. Am J Emerg Med 2011;29:590–3.
7. Jabre P, Leroux B, Brohon S, et al. A comparison of plastic
single-
use with metallic reusable laryngoscope blades for out-of-
hospital
tracheal intubation. Ann Emerg Med 2007;50:258–63.
8. Beleña JM, Gasco C, Polo CE, Vidal A, Núñez M, Lopez-
Timoneda F. Laryngeal mask, laryngeal tube, and Frova
introducer
in simulated difficult airway. J Emerg Med 2015;48:254–9.
9. Dries DJ, Endorf FW. Inhalation injury: epidemiology,
pathology,
treatment strategies. Scand J Trauma Resusc Emerg Med 2013;
21:31.
10. Cancio LC. Airway management and smoke inhalation
injury in the
burn patient. Clin Plast Surg 2009;36:555–67.
11. Evans A, Vaughan RS, Hall JE, Mecklenburgh J, Wilkes
AR. A
comparison of the forces exerted during laryngoscopy using
dispos-
able and non-disposable laryngoscope blades. Anaesthesia
2003;58:
869–73.
24. 12. Scholz A, FarnumN,Wilkes AR, HampsonMA, Hall
JE.Minimum
and optimum light output of Macintosh size 3 laryngoscopy
blades:
a manikin study. Anaesthesia 2007;62:163–8.
13. Buléon C, Parienti JJ, Lesage A, et al. Comparison of
plastic and
metallic single-use and metallic reusable laryngoscope blades: a
randomised controlled trial. Eur J Anaesthesiol 2013;30:163–9.
14. Itoman EM, Kajioka EH, Yamamoto LG. Dental fracture
risk of
metal vs plastic laryngoscope blades in dental models. Am J
Emerg
Med 2005;23:186–9.
15. Goodwin N, Wilkes AR, Hall JE. Flexibility and light
emission of
disposable paediatric Miller 1 laryngoscope blades*.
Anaesthesia
2006;61:792–9.
16. Jabre P, Galinski M, Ricard-Hibon A, et al. Out-of-hospital
tracheal
intubation with single-use versus reusable metal laryngoscope
blades: a multicenter randomized controlled trial. Ann Emerg
Med 2011;57:225–31.
17. Dyson A, Harris J, Bhatia K. Rapidity and accuracy of
tracheal intu-
bation in a mannequin: comparison of the fibreoptic with the
Bul-
lard laryngoscope. Br J Anaesth 1990;65:268–70.
25. 18. Holden JD. Hawthorne effects and research into professional
prac-
tice. J Eval Clin Pract 2001;7:65–70.
Journal Article Grading Rubric
2
1
0
Basic Mechanics
Length 3-4 paragraphs. Reference, and article or URL given.
Technical terminology and formalism are used correctly.
Somewhat too long or short. Reference or article/URL given.
Small number of errors in terminology or formalism.
Much too long or short. No reference or article given.
Terminology, formalism frequently misused.
Understanding of article
Chosen point identified and clearly explained. Factually correct
as report of chosen aspect of article. Explains chosen point;
goes beyond merely paraphrasing or quoting. Class knowledge
used correctly where appropriate.
Chosen point identified, but explanation not fully clear. Minor
errors in report of authors' meaning. Chosen point paraphrased
in student's own words, but very close to original. Minor
misunderstandings related to class knowledge.
No point identified, or explanation very unclear. Major errors in
report of authors' meaning. Relies on quotations or superficial
paraphrase; little evidence of understanding. Major problems
from not applying class knowledge.
Active and critical thinking; argumentation
Goes beyond summary; includes critique, connects to other data
or ideas. Tight focus on main point. Report is well organized;
26. paragraphs and overall discussion is focused, coherent.
Examples, data used appropriately.
Shows understanding of relevant issues, but contributes no
substantial original points. Focus is somewhat loose. Some
organization, but relationships between ideas not always clear.
Crucial examples, data not always given.
Critical discussion missing, or shows serious misunderstanding
of article. No clear focus. Structure of discussion has no clear
organization. Examples used, but not connected to discussion.
Writing
Clear articulate writing used. One or two minor edits needed to
be a perfect paper! Keep up the great work
Edits needed. Proof reading will help you. Read aloud to
yourself and or ask others to read it out loud to you.
Turns in something. Not college level work at all. Get help at
the writing center.
Your Thoughts
Articulates your thoughts on the article in a clear manner.
Discusses what you learned from reading the article or ideas
you might use in the future.
Brief mention of thoughts, but did not elaborate. No mention of
learning from reading the article.
Does not write any of your own thoughts or ideas about what is
discussed in the article.
EDSP 360
Sample Lesson Plan Form
Lesson Plan: Sense of Taste
Name: Dynamic Teacher
27. Course: EDUC 360
LESSON PREPARATION[Before the lesson]
Topic: Sense of Taste
Specific Strategy: Introduction to the definition of taste, the
sensory descriptors, and the body part that helps us taste things.
Subject: Science
Grade: Kindergarten
State Standard:
K.2 Students will investigate and understand that humans have
senses that allow one to seek, find, take in, and react or respond
to information in order to learn about one’s surroundings. Key
concepts include
a) five senses and corresponding sensing organs (taste – tongue,
touch – skin, smell – nose,
hearing – ears, and sight – eyes); and
b) sensory descriptors (sweet, sour, bitter, salty, rough/smooth,
hard/soft, cold, warm, hot,
loud/soft, high/low, bright/dull)
National Standard:
NS.K-4.2 PHYSICAL SCIENCE
As a result of the activities in grades K-4, all students should
develop an understanding of properties of objects and materials.
Primary Objective: Given 6 different pictures, the student will
write the corresponding sensory descriptor (bitter, sweet, sour,
or salty), correctly identifying 4 out of 6 pictures.
Classroom Diversity and Differentiated Instruction: This class
contains 18 Kindergarten students. There is one student who is
Korean, 10 are Caucasian, and 7 are African America. Two
students are advanced, 13 are average, and three are below
28. level. Three students have ADHD, the tasting test for the
different objects will allow for active participation and
increased learning. The poster will also allow for active
participation and increased learning. They will be assessed in a
small group to maintain focus. One student has a hearing
impairment. I wear an amplifier that connects to a headset he
wears to help him hear the lesson. I test this student in a small
group to insure he understands the assessment.
Materials/Equipment:
· Napkins,
· Jelly beans
· Unsweetened chocolate
· 2 Lemons cut into slices
· Pretzels
· Paper
· Pencil
· Crayons
· Poster paper
· Glue stick
· Rius, M., Parramon, J. M., & Puig, J. J. (1986). Taste: The
Five Senses. Barrons Juveniles.
Technology Integration:
The students will use the computer lab to find a picture of each
sensory descriptor (bitter, salty, sweet, and sour). They will
print out a picture of each and use these pictures for their sense
of taste poster.
Character Principle:
“God’s word is important in our daily life. It is important that
29. we live by His word.”
“How sweet are your words to my taste, sweeter than honey to
my mouth!” Psalm 119:103 I will use the Scripture in my set.
LESSON PRESENTATION [during the lesson]
Set:
Read Psalm 119:103. Explain to the class that the book of Psalm
was written by David.
“What did David say was sweet?” (God’s words) “What did
David say they are sweeter than?” (honey) “In Bible times
people used honey as sugar. David said he loved God’s words
more than sweet things.”
“Today we are going to learn about different tastes and how we
use taste to discover about God’s world.”
Teacher Instruction/Modeling:
Instruct the students to pull out their literature book and flip to
pages 10-11. After they have flipped to the correct pages,
instruct them to find a seat on the reading carpet. While
following along in their literature book, the teacher will read
the selection:
Taste is one of your senses.
You use your tongue and mouth to taste.
You taste things that are sweet.
You taste things that are sour.
You taste things that are salty.
You taste things that are bitter.
You use taste to discover about God’s world.
The teacher will then ask the students:
· What part of your body do you use taste? (mouth, tongue)
30. · What are the four kinds of tastes? (sweet, sour, bitter, salty)
· What can taste be used for? (discovering God’s world)
· Which of your senses do you use your tongue and mouth for?
(taste)
· What are some things that taste sweet? (varied responses)
· What are some things that are salty? (varied responses)
· What are some things that are sour? (varied responses)
· What are some things that are bitter? (varied responses)
· What is your favorite taste? (varied responses)
Read the book, Taste: The five Senses, by Maria Rius. Ask the
students what taste is. (One of the senses.) “What do we use
taste for?” (To discover God’s world.) “What kinds of taste are
there?” (bitter, sweet, sour, and salty) Reading the book, the
teacher will stop and point to the picture shown. The students
will determine whether the food is sweet, salty, bitter, or sour.
After the story is finished, the teacher will review the sensory
descriptors.
Guided Student Practice:
After reading the story, the students will go back to their seats
quietly. The teacher will give each student a napkin, jelly bean,
pretzel, lemon slice, and piece of unsweetened chocolate. The
students will be instructed not to touch these items until told to
do so by the teacher. After each student has received their
items, the teacher will label these items on the board and draw a
blank beneath the word. The class will then be instructed to eat
the pretzel. The teacher will ask: How does this pretzel taste?
(salty) Why do you think this pretzel tastes salty? (because it
has salt on it) The teacher will then write the word salty beneath
31. the word pretzel. The teacher will then instruct the students to
taste the lemon slice. The teacher will ask: How does this lemon
slice taste? (sour) Why do you think this lemon slice tastes
sour? (the juice) The teacher will then write the word sour
beneath the word lemon slice. The teacher will then instruct the
students to eat the unsweetened chocolate. The teacher will ask:
How does this piece of chocolate taste? (bitter) Why do you
think this piece of chocolate tastes bitter? (because it doesn’t
have any sugar) The teacher will then write the word bitter
beneath the word unsweetened chocolate. The teacher will then
instruct the students to eat the jelly bean. The teacher will then
ask: How does this jelly bean taste? (sweet) Why do you think
this jelly bean tastes sweet? (because it has sugar in it) The
teacher will then write the word sweet beneath the word jelly
bean.
Independent Student Practice:
After the students complete their class experiment, they will
clean up their area. After they are finished cleaning their area,
the students will then be called to line up to go to the computer
lab. At the computer lab, each student will find a picture of
each sensory descriptor (bitter, sweet, salty, and sour). They
will be given 15 minutes to find 4 pictures. After the student
has found their picture, they will print these pictures out. The
class will then go back to the classroom. The teacher will
distribute a piece of poster paper to each student. Each student
will be given 20 minutes to complete a poster of the different
sensory descriptors. They will glue their pictures to the poster
and write the corresponding sensory descriptor next to it. After
they have glued and labeled their pictures, they will write why
they like or dislike this item. After the class is finished with
their independent poster projects, the students will share them
with the class.
Closure:
“Today we learned about taste! What is taste?” (a sense) “What
do we use to taste?” (tongue/mouth) “What are the 4 different
sensory descriptors for taste?” (bitter, sweet, sour, and salty)
32. “What are some things that are sweet?” (varied answers) “What
are some things that are bitter?” (varied answers) “What are
some things that are salty?” (varied answers) “What are some
things that are sour?” (varied answers)
“Is God’s word sweet, sour, bitter, or salty?” (sweet) “What is
God’s word sweet like?” (honey) “God’s word is important. It is
important that we use God’s word to be sweet and kind to
everyone.”
Summative Assessment:
The teacher will pass out a worksheet. This worksheet will have
6 different pictures on it. There will be a picture of a lollipop, a
pretzel, a cookie, coffee, a cracker, and a lemon. The students
will be given 15 minutes to write the corresponding sensory
descriptor. The words will be on the board so the student can
correctly write the word next to the corresponding item. After a
student has finished, they may color the pictures.
EDSP 360
Standard Lesson Plan Form
Lesson Plan:
Name:
Course: EDSP 360
LESSON PREPARATION[Before the lesson]
Topic:
Specific Strategy:
Subject:
Grade:
State Standard:
National Standard:
Primary Objective:
Classroom Diversity and Differentiated Instruction:
33. Materials/Equipment:
Technology Integration:
Character Principle:
LESSON PRESENTATION [during the lesson]
Set:
Teacher Instruction/Modeling:
Guided Student Practice:
Independent Student Practice:
Closure:
Summative Assessment:
EDSP 360
Standard Lesson Plan Form
Lesson Plan:
Name
:
Course
:
EDSP 360
LESSON PREPARATION
[Before the lesson]
Topic
:
35. [during the lesson]
Set
:
Teacher Instruction/Modeling
:
Guided Student Practice
:
Independent Student Practice:
Closure
:
Summative Assessment
:
EDSP 360
Standard Lesson Plan Form
Lesson Plan:
Name:
Course: EDSP 360
LESSON PREPARATION [Before the lesson]
Topic:
Specific Strategy:
Subject:
Grade:
State Standard:
36. National Standard:
Primary Objective:
Classroom Diversity and Differentiated Instruction:
Materials/Equipment:
Technology Integration:
Character Principle:
LESSON PRESENTATION [during the lesson]
Set:
Teacher Instruction/Modeling:
Guided Student Practice:
Independent Student Practice:
Closure:
Summative Assessment:
EDSP 360
Standard Lesson Plan Instructions
** TEACH IT, PRACTICE IT, TEST IT! **
Lesson Plan #__: __________
Name:
Course: EDSP 360
LESSON PREPARATION[before the lesson]
Topic: Correct subject/grade/topic and are age appropriate.
Concept:
Subject:
Grade:
State Standard[Virginia SOL or reading standard of your state]:
Virginia SOLs can be located at http://www.pen.k12.va.us/
National Standard National Standards can be found at
37. http://www.educationworld.com/standards/national/toc/index.sh
tm
Primary Objective[Objective must match Summative
Assessment below.]
Must be a specific statement which provides a basis for
evaluating whether or not the objective was accomplished, by
each individual student (measured by the summative
assessment). The objective should describe the skill to be
taught, not the content to be used. The following components
must be stated in each objective:
Condition of the task: for example, "Given ten vocabulary
words..." -- not "After a vocabulary lesson."
Learner: Be specific. "each student” or “students in group 3”
Performance/Observable task: Must be a verb that can be
observed -- not "know" or "understand"
Criterion (MEASURABLE): For example, "state three reasons,"
"draw one picture," "answer 18 of the 20 correctly" Do not use
percentages in lesson plan objectives.
Sample objectives:
Given 10 vocabulary words, each student writes a correct
definition for at least 9 of the words.
In an essay, each student in group two writes an essay
integrating each of 10 teacher identified vocabulary words with
contextual accuracy.
Classroom Diversity and Differentiated Instruction[Describe
student diversity and related aspects of lesson and how
instruction will be adapted]
Description of the group for whom the lesson is being prepared.
Identify cultural groups, learning style groups, ability groups,
and any special needs groups represented. Define any special
groupings to be addressed during the lesson. Describe the
38. student diversity and related aspects of lesson and how the
lesson will be adapted to accommodate the diverse learners.
For this course, mention the disabilities and how you alter the
lesson to reach those students with the disabilities.
Materials/Equipment[Be creative! Manipulative activity
required]
List the materials and equipment needed for the lesson. Be
creative! Include authentic children's literature: poetry, drama,
fiction, nonfiction, and research materials suitable to the
content area of study. Or perhaps manipulatives, maps,
samples, etc. Be sure to list printed materials in APA format.
Technology Integration[Provide software title or website that
could be used for this topic]
Hardware/software used by teacher and/or students and how it
will be integrated into the lesson. Specify the net address for
each entry.
Character Principle[Choose character principle related to
children’s literature selection.]
Choose a character trait that applies to the lesson. State the
principle in student terms, a correlated verse, and the scripture
reference. Explain how this will be used in the lesson.
LESSON PRESENTATION [during the lesson] The following
steps are designed to prepare students to be successful in the
summative evaluation at the end of the lesson.
Set[Introduce lesson concept.]
Introductory activity to get students' attention and focus
attention on the lesson topic.
Teacher Instruction[Explain lesson concept.]Teacher
Modeling[Demonstrate examples of lesson concept.]
Include a brief explanation of the concept to be taught and one
or more examples to be modeled by the teacher. If steps or
skills are part of the lesson, list the steps or skills. This needs
to be explained in the detail that a reader will know that you
39. understand the concept being taught.
Guided Student Practice[formative assessment]:
Students practice additional examples with the teacher's
guidance using an activity, assignment, or experience. Group
activities are appropriate. Teacher observes student performance
(formative assessment).
Independent Student Practice[formative assessment – practice
for summative assessment]:
Once the teacher is satisfied that the students understand the
examples completed as a group with teacher guidance,
additional examples are assigned to be completed
independently. The teacher should circulate through the room to
observe whether students are having difficulty and help them as
needed (formative assessment). This is not the same as the
summative assessment not is this where you evaluate the
objective. Rather it is practice for the summative assessment.
Closure[Review lesson concept and character principle.]
Review the concept taught. (Restate the objective and/or ask
students.) Summarize and solidify.
Summative Assessment[Measure performance of each individual
student]:
Must measure the objective stated in the lesson plan. (How will
you grade or check to see if the objective was achieved?)
Example: Student quiz, student writing, or checklist (marked by
the teacher, student, or peer) to assess each student's
performance. This is not the same as the independent practice.
DO NOT ASSIGN HOMEWORK unless the students
demonstrate mastery. The parents are important in the lives of
their children, but YOU are the teacher.