Artifacts in Nuclear Medicine with Identifying and resolving artifacts.
arterial pulse.pptx
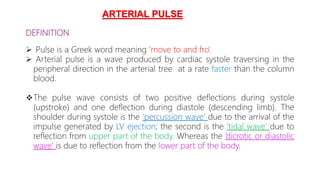
1. DEFINITION
Pulse is a Greek word meaning ‘move to and fro’.
Arterial pulse is a wave produced by cardiac systole traversing in the
peripheral direction in the arterial tree at a rate faster than the column
blood.
The pulse wave consists of two positive deflections during systole
(upstroke) and one deflection during diastole (descending limb). The
shoulder during systole is the ‘percussion wave’ due to the arrival of the
impulse generated by LV ejection; the second is the ‘tidal wave’ due to
reflection from upper part of the body. Whereas the ‘dicrotic or diastolic
wave’ is due to reflection from the lower part of the body.
ARTERIAL PULSE
5. As the normal aortic pulse wave is transmitted peripherally
(reaches carotid at 30 ms, brachial 60 ms, radial 80 ms, and
femoral at 75 ms).
Normally, percussion wave is more prominent than tidal wave.
However; in older patients with increased systemic vascular
resistance, arteriosclerosis and diabetes mellitus, the tidal wave
may be somewhat higher than the percussion wave (i.e. late
systolic peak).
The height of the dicrotic wave decreases with age,
hypertension and arteriosclerosis.
6. EXAMINATION OF THE ARTERIAL PULSE
Ejection of blood with every cardiac contraction is converted into:
i. Flow pulsations: i.e. longitudinal movement of blood along the arterial lumen
which can be measured by electromagnetic flow meters and Doppler ultrasonic
probe.
ii. Pressure pulsations: The amplitude of the arterial pulse perceived by the clinician
in a large accessible artery is the pressure pulse.
All major arterial pulses should be bilaterally examined for:
● Rate of the pulse
● Rhythm
● Character
● Volume
● Condition of the arterial wall (thickness)
● Equal (synchronous) or inequality of the radial pulses and
● Presence or absence of delay of the femoral pulses compared with radials.
7. The radial pulse is felt with the tips of the fingers (preferably three: index, middle,
and ring) compressing the vessel against the head of the radius, with the patient’s
forearm slightly pronated and the wrist slightly flexed.
8. The brachial artery is compressed against the humerus just above the antecubital
fossa. The examiner should use either the left thumb or fingertips when examining
patient’s right brachial artery and vice versa.
9. The carotid (common carotid) is gently examined one at a time best with the
thumb (left thumb for patient’s right carotid and vice versa) with the
sternocleidomastoid muscles relaxed and the head rotated slightly towards the
examiner. It should be palpated in the lower half of the patient’s neck in order to
avoid carotid sinus compression.
10. The femoral arteries lie midway between the iliac crest and pubic ramus and
are palpable against the underlying femur.
11. The popliteals are best examined with the patient’s knee flexed at an angle
of 120. The fingertips of both hands are placed in the popliteal fossa with
thumbs resting on the patient’s patella.
12. The posterior tibial pulse is found 1 cm behind the medial malleolus
of the tibia. The patient’s foot should be relaxed between plantar and
dorsiflexion.
13. The dorsalis pedis pulse is commonly felt between the tendons of 1st and 2nd
toes, 5–7.5 cm below the joint crevice. It is compressed against the tarsal bones
the patient’s left dorsalis pedis is mostly examined with the fingers of the right
and vice versa.
14. The examination of the arterial pulses is tabulated using a
scale as follows:
0=Complete absence of pulsation.
1+ =Small or feeble/reduced pulsation.
2+ =Palpable but diminished as compared to other side.
3+ = Normal pulsation.
4+ = Large or high volume/bounding pulsation.
15. Rate of the Pulse
Examine whether the patient has tachycardia, bradycardia or
pulse deficit.
The range of rates of normal sinus rhythm in an adult
is between 60 and 100 beats per minute.
However, the average rate of pulse in children depends
the age and is as follows: 1 week of age 140/min, 1 yr of age
120/min, 6 yrs of age 100/min and at puberty 80/min.
16. Pulse Deficit
The difference between the radial pulse rate and the heart rate (usually
counted by auscultation) is defined as pulse deficit.
A pulse deficit of > 6/min is diagnostic of atrial fibrillation and < 6/min
can occur in premature ventricular contractions (PVCs).
Mechanism of pulse deficit
● In tachyarrhythmias, the diastole is shortened and subsequent systolic
stroke volume is insufficient to cause opening of the aortic valve
the arterial pulse will be non-existent inspite of the cardiac contraction.
● As diastole becomes longer in subsequent cardiac cycles, the stroke
volume gradually increases and arterial pulse is felt.
17. Rhythm
The normal pulse is regular in rhythm. If the pulse is irregular,
note whether it is regularly irregular or irregularly irregular.
18. Character of the Pulse
It is best evaluated by palpation of the carotid pulse. Following are the
abnormal types of pulses depending upon the character of the pulse:
(1) Pulsus Tardus (Slow Rising Pulse)
Slow rising pulse with delayed systolic peak (nearer to S2) and upstroke,
frequently associated with a thrill in the carotids (carotid shudder) is
characteristic of AS, and often occurs with pulsus parvus (i.e. pulsus parvus
et tardus).
It is better appreciated by simultaneous auscultation and carotid palpation.
19. (2) Water-Hammer (Collapsing) Pulse or Corrigan Pulse or Pulsus Celer:
It is characterized by rapid upstroke (percussion wave) followed by rapid descent
(collapse) of the pulse wave without dicrotic notch, which reflects low systemic vascular
resistance.
Rapid upstroke is due to the rapid ejection of greatly increased stroke volume.
The rapid descent or collapsing character is due to:
(i) Diastolic ‘run-off ’ (back flow) into the left ventricle.
(ii) Reflex vasodilatation mediated by carotid baroreceptors secondary to large stroke
volume.
(iii) The rapid run-off to the periphery due to decreased systemic vascular resistance.
20.
21. CAUSES
i) Conditions with aortic run-off: AR, PDA, AP window, rupture of sinus of
Valsalva into the right chambers and arteriovenous fistula.
ii) Cyanotic congenital heart diseases: Truncus arteriosis with truncal run-
off into PA or truncal insufficiency, pulmonary atresia with
bronchopulmonary collaterals, TOF with bronchopulmonary
collaterals/associated PDA/associated AR or after Blalock Taussig (BT)
(systemic artery to pulmonary artery).
iii) Hyperkinetic circulatory states: Pregnancy, anemia, thyrotoxicosis,
Beriberi, fever and Paget’s disease of the bone .
23. Anacrotic pulse:
In the slow rising pulse (pulsus tardus), a distinct notch (anacrotic) on the
upstroke of the carotid pulse with two separate waves (anacrotic and
percussion) can be palpated.
This is characteristically found in AS.
Lower the notch, severe is the AS, and the presence of anacrotic pulse
indicates 70mmHg pressure gradient.
24.
25. Bisferiens Pulse :
It is characterized by two systolic peaks (percussion and tidal waves)
separated by a distinct midsystolic dip.
26. Causes and mechanism of bisferiens pulse:
i) Conditions with large stroke volume:
It occurs in conditions in which a large stroke volume is rapidly ejected from
the LV as in severe AR, PDA, hyperkinetic circulatory states.
Normally, the percussion wave is felt but not the tidal wave (these waves are
due to the elastic recoil of aorta and reflected wave from the periphery
respectively). Hence in situations where the initial percussion wave is
exaggerated due to large stroke volume (as in severe AR), the tidal wave also
becomes prominent.
ii) Combination of slow rising and collapsing pulse:
Bisferiens pulse also occurs in patients with combined AS and AR, a
combination of slow rising and collapsing pulses.
The stenosis permits a jet lateral to the increased velocity of jet which causes a
fall in pressure (Bernoulli phenomenon) and results in a dip in the pulse wave
with a secondary outward movement (prominent tidal wave).
27. Hypertrophic obstructive cardiomyopathy (HOCM):
Bisferiens pulse may also occur in HOCM. However, it is usually recordable but
palpable.
The initial percussion wave is due to rapid ejection of blood into the ascending
aorta during early systole.
The midsystolic dip (negative wave) coincides with marked decrease in the rate
LV ejection, as the left ventricular outflow tract obstruction becomes manifest
to the thickening of interventricular septum and the systolic anterior motion
(SAM) of anterior mitral leaflet.
The second systolic (tidal) wave is most likely produced by reflected waves from
the periphery.
Hence, pulse of HOCM behaves partly like AR (initial
and partly as AS (second component), but percussion wave is more prominent
the tidal wave.
28. Detection:
It is readily detected by palpating the carotids.
● However, the presence of carotid systolic thrill may mask the
features of bisferiens pulse, in which case peripheral pulses like
radial or brachial are suitable for detection of this pulse.
● Apply graduated pressure or completely obliterate the pulse
gradually release it to appreciate the two waves.
29. Dicrotic pulse
It is characterized by two peaks, one in systole (percussion wave) and the other in
diastole (dicrotic wave) immediately after S2, which is due to accentuated and
palpable reflected wave from the periphery.
30. Commonly seen in low output states such as:
Cardiomyopathy
Cardiac tamponade
Myocarditis
Hypovolemic shock and
During intraoartic balloon pump (IABP).
Enteric fever or any fever with vasodilatation due to the circulating vascular
toxins.
31. Detection:
It can be felt in carotids, but can be better appreciated in the radial
artery.
It is better appreciated during inspiration and with the inhalation of
amylnitrate.
Simultaneous auscultation is helpful as it occurs immediately after S2.
32. (4) Irregularly Regular Pulse
It consists of pulsus bigeminus and pulsus alternans.
(i) Pulsus bigeminus: It is an irregular rhythm caused by premature contractions (usually PVCs)
resulting in the alteration of the strength of the pulse which may be confused with pulsus
alternans.
● However, in pulsus bigeminus, the weak beat always follows the short interval and the long
compensatory pause following a premature beat is followed by a stronger than normal pulse
normal individuals or in states of fixed left ventricular outflow tract obstruction such as AS.
● Stronger pulse is due to more diastolic filling following long compensatory pause and
extrasystolic potentiation of ventricular contraction.
● Pulsus bigeminus may also be seen in AV blocks and atrial flutter with block.
33. Pulsus alternans:
It is a regular rhythm in which a strong beat alternates with a weak beat
is related to alternating more number of contractile elements and loss of
contractile elements participating in each contraction.
It is frequently precipitated by PVCs and is a sign of severe LV dysfunction.
34. Causes
● Severe AS (often with failure)
● Dilated cardiomyopathy, myocarditis
● Acute pulmonary embolism and severe pulmonary stenosis.
Detection: It is better appreciated in the peripheral pulses (radial and femoral).
35. Pulsus alternans:
Types
● Total: When the weak beat is not perceived at all or when involving both sides of the
heart.
● Partial: When involving only RV (as in PE) or LV (as in AS).
● Right atrial pulsus alternans: Severe right ventricular failure rarely associated with
tall ‘a’ and ‘v’ waves that alternate with short ‘a’ and ‘v’ waves of right atrial pressure.
● Compound pulsus alternans: Additional alteration involving the weak beats in
association with a usual alteration of strong and weak beats is said to have compound
pulsus alternans.
36. (5) Pulsus Paradoxus
It is defined as an exaggerated decrease in the strength (amplitude) of the
pulse during normal quiet inspiration due to the exaggeration of normal
inspiratory decline in the systolic arterial pressure of 10 mmHg, reflecting an
exaggerated inspiratory decline of 7% in the LV stroke volume.
38. Detection:
● When the inspiratory decline of systolic arterial pressure is 20 mmHg, pulsus
paradoxus is easily detected by the palpation of radial or brachial artery as an
inspiratory decline in the amplitude of the pulse.
● Milder degrees of paradoxical pulse can be readily detected by
sphygmomanometry.
The cuff should be inflated 20 mmHg above the systolic pressure and slowly
deflated at a rate of 2 mmHg/heart beat, when the Korotkoff sounds are heard
during expiration (i.e. peak systolic pressure during expiration). The cuff is further
deflated more slowly to the point at which Korotkoff sounds are heard equally well
in both inspiration and expiration. The difference between these two pressures is
estimated magnitude of pulsus paradoxus. The patient should be breathing
and should not take a deep breath as normal individuals can have pulsus
with deep breathing.
39. Mechanism of pulsus paradoxus
● Normally, inspiration results in fall of intrapericardial pressure (IPP
, from 3mmHg
to 6 mmHg) which causes increase of right ventricular transmural pressure and
venous return with slight changes in right and left ventricular sizes.
● In pulsus paradoxus inspiration causes a decline in elevated intrapericardial
(often from 20 mmHg to 18 mmHg) and right atrial pressure that results in the
increase of RV transmural (distending) diastolic pressure which augments the venous
return and the filling of the right heart.
This in turn results in:
(1) The increase in RV (diastolic) dimensions producing flattening and leftwards
shift of the interventricular septum thereby compressing the LV (i.e. ⇓ LV
dimensions and compliance) that impedes LV filling and decreases LV output
and systolic arterial pressure.
(2) The increase of intrapericardial pressure and fall of the LV transmural diastolic
pressure which further impedes LA and LV filling, fall in LV output and decrease
of systolic arterial pressure
● This can be substantiated by echocardiography.
40.
41. Additional factors for pulsus paradoxus
● Inspiratory pooling of blood in the pulmonary bed (pulmonary veins and
(i.e. increase of hang out interval) produces decline in LA and LV filling and LV
stroke volume and systolic arterial pressure.
● The underfilled LV (LV volume is decreased in cardiac tamponade) may be
in the steep ascending limb of Starling curve so that any inspiratory reduction of LV
filling results in marked depression of the LV stroke volume and the systolic
pressure.
Pulsus paradoxus in COPD: The decrease in lung compliance magnifies the normal
inspiratory decrease in LV volume and systolic arterial pressure and expiration may be
accompanied by an excessive rise in the systolic pressure above normal.
42. Absence of pulsus paradoxus:
Pulsus paradoxus is absent, when cardiac tamponade (CT) occurs in a condition
which permits equal filling of both ventricles (e.g. shunt) or more filling of LV (e.g.
AR).
CT without pulsus paradoxus occurs when associated with:
● ASD due to equal filling of both ventricles in both phases of respiration
● VSD due to free communication between the ventricles preventing differential
filling
● AR as filling of LV is maintained irrespective of respiration
● Pericardial adhesions especially over the right side of the heart.
43. Types
(i) Total paradox is the complete disappearance of palpated pulse during
inspiration, which occurs during very severe CT or CT combined with hypovolemia.
(ii) Reversed pulsus paradoxus: There is an inspiratory increase and an expiratory
decrease of systolic arterial pressure. It occurs in:
● Positive pressure breathing with artificial ventilators: Intrathoracic pressure is
higher during inspiration and lower during expiration i.e. reversal of the normal.
If CT occurs in this setting, reversal of pulsus paradoxus is noted.
● Isorhythmic AV dissociation: (atrial activity precedes QRS during inspiration
and marches into QRS during expiration) The atrial activity during inspiration
increases the stroke volume and its lack during expiration decreases the stroke
volume and systolic pressure.
● HOCM: Reversed pulsus paradoxus occurs in HOCM, but the mechanism is
not known.
44.
45. Volume of the Pulse
It gives an idea of the pulse pressure, which depends on the stroke volume
and the compliance of the arteries. The pulse volume could be normal, low
high. Pulsus parvus, pulsus magnus and hyperkinetic pulse are the types of
pulse depending upon its volume.
46. Pulsus Parvus
It is a low volume small amplitude pulse (a small weak pulse) that occurs
of the decreased stroke volume, characteristically seen in AS with pulsus tardus.
● Pulsus parvus et tardus refers to a small pulse with a delayed systolic peak
characteristic of severe AS.
● Pulsus parvus is also observed in severe heart failure.
● It is best detected by palpating the carotids.
47. Pulsus Magnus
It is a high volume large amplitude pulse because of an
stroke volume, characteristically seen in AR.
48. Hyperkinetic or Bounding Pulse
It is characterized by a large bounding pulse due to an increased stroke
volume and rapid ejection from the left ventricle.
● It occurs in patients with elevated stroke volume, sympathetic
and in patients with a rigid sclerotic aorta. It is typically seen in
circulatory states.
● In MR and VSD, the forward stroke volume (from LV into aorta) is usually
normal, but the fraction ejected during early systole is greater than
Therefore, the pulse is of normal volume but may rise briskly (also
as abnormally rapid).
49. Condition of the Vessel Wall
It is examined by flattening the artery by digital pressure and
it sideways.
● Atherosclerotic vessel is thickened, rigid and tube like.
● It is hard and calcified in Monckeberg’s degeneration (medial
calcification).
50. Radial Pulse Synchronicity
Examine whether the radial pulses are equal on both sides. Radial pulse on one
may be diminished or absent in patients with:
● Takayasu arteritis
● Thoracic outlet syndrome (commonly a cervical rib, scalenus anticus syndrome)
● Subclavian steal syndrome
● Chronic atherosclerosis (predominantly involves innominate, more commonly the
left subclavian artery)
● Acute microemboli to the arm from the heart or from proximal aneurysmal lesion
(including aortic aneurysm)
● Coarctation of aorta (if proximal vessels are also involved) and
● Dissection of aorta.
51. Absent or Delayed Femoral Pulsations
While palpating radial pulse, place fingers of the other hand over the femoral pulse
(below inguinal ligament, one third of distance from pubic tubercle).
A noticeable delay in the arrival of femoral pulse is suggestive of:
● Coarctation of aorta (COA): In COA, the radiofemoral delay is not due to the delay in
time but due to the delay in its rate of rise (amplitude).
● Occlusive disease of the bifurcation of the aorta, common iliac or external iliac arteries.
52. CHARACTERISTIC FEATURES OF PULSE IN COMMON CLINICAL
CONDITIONS
Aortic Stenosis (AS)
Following are the characteristic features of the pulse in aoric stenosis:
● Pulsus parvus et tardus: This is a low volume and slow rising pulse with
delayed systolic peak characteristic of severe AS.
● Anacrotic pulse: In slow rising pulse, a distinct notch (anacrotic) on the
upstroke of the carotid pulse with two separate waves (anacrotic and
percussion).
● Pulsus alternans: It occurs in severe AS.
● Pulsus bisferiens: It occurs in patients with combined AS and AR, a
combination of slow rising and collapsing pulses in which the two waves
(percussion and tidal) are equal or tidal wave may be prominent.
53. Aortic Regurgitation (AR)
● Water hammer (collapsing) pulse:
It is characterized by rapid upstroke followed by rapid descent of the pulse wave
and is best appreciated at the radial pulse (see Figs 14.11 and 14.12).
● Pulsus bisferiens: It is characterized by two systolic peaks separated by a distinct
mid systolic dip. Either the percussion and tidal waves are equal or the tidal waves
is prominent. It is readily detected by palpating the carotids. Its presence indicates
severe AR.
● Pulsus magnus: It is a high volume large amplitude pulse, and is best detected
the radial pulse. Its presence indicates mod-severe AR.