

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Acute rheumatic fever
Similar to Acute rheumatic fever (20)
More from PDT DM CARDIOLOGY
More from PDT DM CARDIOLOGY (20)
Recently uploaded
Recently uploaded (20)
Acute rheumatic fever
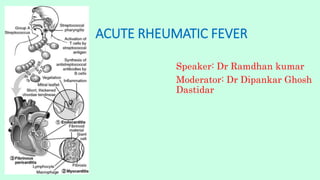
- 1. ACUTE RHEUMATIC FEVER Speaker: Dr Ramdhan kumar Moderator: Dr Dipankar Ghosh Dastidar
- 2. ACUTE RHEUMATIC FEVER It is multisystem disease. ARF results from an autoimmune response to infection with group A streptococcus. Major effect on health is due to damage to heart valves.
- 3. Occurring most often between 5 and 15 years. The inflammatory process causes damage to collagen fibrils and connective tissue ground substance, resulting in combinations of Arthritis, Carditis, Erythema marginatum, Subcutaneous nodules, and Chorea. The French physician Ernst-Charles Lasegue famously said, in 1884, that “rheumatic fever licks the joints but bites the heart.”
- 4. EPIDEMIOLOGY TheWorldwide, incidence is 19/100,000 (range, 5 to 51/100,000), with lowest rates (<10/100,000) in North America and Western Europe and highest rates (>10/100,000) in Eastern Europe, the Middle East, Asia, Africa, Australia, and New Zealand.2
- 7. Its occurrence is similar between women and men, the inherent biological factors, the risk of illness during pregnancy, exposure to GAS through child rearing, and poor accessibility to resources make women approximately 1.8 times more susceptible to developing RHD.3
- 8. PATHOGENESIS RF is a multifactorial disease that follows GAS (the agent) pharyngitis in a susceptible individual (the host) who lives under deprived social conditions (the environment). The theory of molecular mimicry hold that GAS pharyngitis triggers an autoimmune response in susceptible individuals by cross-reacting with similar epitopes in the heart, brain, joints, and skin, and that repeated episodes of RF lead to RHD. In situations of untreated epidemic GAS pharyngitis, up to 3% of patients develop the disease.
- 9. THE HYPOTHESIS OF MOLECULAR MIMICRY: In the pathogenesis of RF1 state that patients with RHD have cross-reactive autoantibodies that target the dominant GAS epitope of the group A carbohydrate, N- acetyl-beta-d-glucosamine (GlcNAc), and laminin and laminar basement membrane in heart valve endothelium. T cells in peripheral blood and heart valves of RHD patients cross-react with streptococcal M protein and cardiac myosin.
- 10. THE TWO-HIT HYPOTHESIS: For the initiation of disease proposes that antibody attack of valve endothelium facilitates the extravasation of T cells through activated epithelium into valve tissue, leading to the formation of granulomatous nodules called Aschoff bodies, characteristic of rheumatic myocarditis .The area of central necrosis is surrounded by a ring of plump histiocytes, called Anitschkow cells. These nodules were discovered by Ludwig Aschoff and Paul Rudolf Geipel and thus are occasionally called Aschoff-
- 15. DIAGNOSIS OF ACUTE RHEUMATIC FEVER
- 16. Revised Jones Criteria The 2015 revised Jones criteria incorporate subclinical valvulitis detected by echocardiography is accepted as a major criterion for the diagnosis of ARF in all patient populations for the first time. Two sets of criteria introduced based on population risk; LOW RISK POPULATION: ARF incidence <2/100,000 school age children per year or RHD prevalence of <1/1000. MODERATE AND HIGH RISK: ARF incidence_>2/100,000school age children per year or an all age RHD prevalence of >1 /1000.
- 18. POLYARTHRITIS
- 19. POLYARTHRITIS Most common manifestation (65-75%) More common and more severe in young adults (100%), teenagers (82%), and children (66%). Asymmetric, migratory, non suppurative and self limited. In some cases involvement may be additive rather than migratory, with several joints affected simultaneously. Large joints involved (knee, ankle, elbow, and wrist) Shoulder, hip, and small joints of hands and feet may also involved, but almost never alone. If vertebral joints are affected, another disorder should be suspected. It resolve completely, if the joint swelling persist after 4 weeks, consider other condition, such as JIA or SLE. Salicylates and NSAIDS produce a marked and promt relief. MONOARTHRITIS: Occurs in high risk indigenous population (e.g. in India ,Australia, Fiji)- 17 to 25% of patiants.
- 20. Jaccoud arthritis or arthropathy (or chronic post-RF arthropathy): Is a rare manifestation of RF characterized by deformities of the fingers and toes. The condition may occur after repeated attacks of RF and results from recurrent inflammation of the fibrous articular capsule. There is ulnar deviation of the fingers, especially the fourth and fifth fingers, flexion of the metacarpophalangeal joints, and hyperextension of the proximal interphalangeal joints (i.e., swan neck deformity). The hand is usually painless, and there are no signs of inflammation. The deformities usually correctible but may become fixed in the later stages. There are no true erosions on radiography, and the rheumatoid factor is usually negative.
- 22. Poststreptococcal reactive arthritis (PSRA): Is diagnosed in patients who have arthritis that is not typical of RF but who have evidence of recent streptococcal infection. This condition occurs after a shorter latent period than RF, is less responsive to NSAIDs, may be associated with renal manifestations, and evidence of carditis is infrequent. The distinction between PSRA and RF is unclear, and many would recommend that a diagnosis of PSRA not be made in populations where RF is common. Even if the diagnosis is considered, it is appropriate to offer a period of secondary prophylaxis with penicillin, as for episodes of acute RF, in such populations.
- 23. Carditis The incidence of carditis during the initial attack of RF varies from 40% to 91%. Carditis is the most serious manifestation of RF because it may lead to chronic RHD. It may be asymptomatic and detected during clinical examination of patients with arthritis or chorea. Heart failure results from a combination of carditis and valvular dysfunction and occurs in 5% to 10% of the initial episodes, more frequently during recurrences of RF. Patients may have high fever, chest pain, or both; tachycardia is common, especially during sleep. In about 50% of cases, cardiac damage (i.e., persistent valve dysfunction) occurs much later. The symptoms and signs depend on whether there is involvement of the pericardium, myocardium, or heart valves. Valvulitis is the most consistent feature of ARF, and if it is not present, the diagnosis should be
- 28. Echocardiography is recommended for all patients with suspected or definite ARF, as it is more sensitive and specific than cardiac auscultation for detection of acute rheumatic carditis.
- 31. A score of 5 or more was found to be best threshold for diagnosis of carditis (ROC AUC 0.87, sensitivity 76%, specificity 79%).
- 35. Sydenham Chorea Sydenham chorea, also referred to as St. Vitus dance, consists of rapid, involuntary, purposeless, and irregular jerking movements that may begin in the hands but often become generalized, involving the feet and face and interfering with voluntary activity; they disappear during sleep. The CNS is affected in up to 40% of children with RF,23 predominating in females after puberty. The latent period between GAS pharyngitis and chorea is longer (6 to 8 weeks) than for arthritis and carditis; its onset is typically insidious and may be preceded by inappropriate laughing or crying. It can last for up to 2 years (usually 8 to 15 weeks); if it occurs in isolation, all inflammatory markers may be normal and the diagnosis may be overlooked as an indicator of ARF. It does not occur simultaneously with arthritis but may coexist with carditis. Usally self-limiting.
- 37. Cutaneous and Subcutaneous Features Rarely, subcutaneous nodules and erythema marginatum develop in patients already having carditis, arthritis, or chorea; They almost never occur alone. Subcutaneous nodules Occur most frequently on the extensor surfaces of large joints. They may be detected over the occiput, elbows, knees, ankles, and Achilles tendons. Ordinarily, the nodules are firm, painless, and freely movable over the subcutaneous tissue; They vary in size from 0.5 to 2 cm and tend to occur in crops that may be related to the severity of the carditis. They are transitory (seldom more than 1 month) and respond to treatment of joint or heart inflammation.
- 38. Erythema Marginatum Painless rash in fewer than 6% of children. The rash usually appears on the trunk and proximal extremities but not on the face. It is evanescent, pink, and nonpruritic. It extends centrifugally. It sometimes lasts less than 1 day and may become more prominent after a shower/hot bath.
- 42. Differential Diagnosis JIA (especially systemic and, less so, polyarticular), Lyme disease, Reactive arthritis, Arthropathy of sickle cell disease, Leukemia or other cancer, SLE, Embolic bacterial endocarditis, Serum sickness, Kawasaki disease, Drug reactions, Diurnal variation of the fever, evanescent rash, and prolonged symptomatic joint inflammation usually distinguish systemic JIA from ARF.
- 43. NATURAL HISTORY Patients who have had RF have about a 50% likelihood of having a recurrence if they have another episode of untreated GAS pharyngitis. In endemic areas for RHD it is usual to see patients with severe RHD and superimposed ARF, particularly carditis. Episodes of Sydenham chorea usually last several months and resolve completely in most patients, but about one-third of patients have recurrences. Joint inflammation may take one month to subside if not treated but does not lead to residual damage. Prognosis following an episode of ARF depends mostly on how severely the heart is affected, and whether it is a recurrent episode of ARF. Murmurs disappear in about half of patients whose acute episodes were manifested by mild carditis without major cardiac enlargement or decompensation; however, chronic valvular disease can occur, typically over years or decades, in patients who recovered from the acute episode with no evidence of valvular disease. Chronic RHD is the cause of 25% to 45% of all cardiovascular disease and a major cause of heart failure in developing countries.
- 55. INJECTABLE VS ORAL PENCILLIN……
- 59. THANK YOU