Bacterial conjunctivitis Pharmacotherapy
•Download as PPTX, PDF•
21 likes•8,374 views

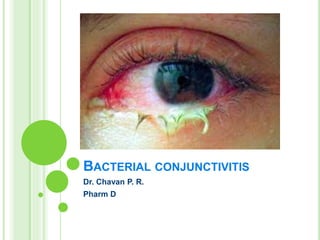
Bacterial conjunctivitis is a common type of pink eye, caused by bacteria that infect the eye through various sources of contamination. The bacteria can be spread through contact with an infected individual, exposure to contaminated surfaces or through other means such as sinus or ear infections.The most common types of bacteria that causes bacterial conjunctivitis includes Staphylococcus aureus, Haemophilus influenzae, Streptococcus pneumoniae and Pseudomonas aeruginosa. Bacterial conjunctivitis usually produces a thick eye discharge or pus and can affect one or both eyes.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Bacterial conjunctivitis Pharmacotherapy
Similar to Bacterial conjunctivitis Pharmacotherapy (20)
More from PranatiChavan
More from PranatiChavan (20)
Recently uploaded
Recently uploaded (20)
Bacterial conjunctivitis Pharmacotherapy
- 1. BACTERIAL CONJUNCTIVITIS Dr. Chavan P. R. Pharm D
- 2. CONJUNCTIVITIS CLASSIFICATION 1. Infective conjunctivitis: bacterial, chlamydial, viral,fungal, rickettsial, spiro chaetal, protozoal, parasitic etc. 2. Allergic conjunctivitis. 3. Irritative conjunctivitis. 4. Keratoconjunctivitis associated with diseases of skin and mucous membrane. 5. Traumatic conjunctivitis. 6. Keratoconjunctivitis of unknown etiology. eg: Trachoma
- 3. INFECTIVE CONJUNCTIVITIS It is of following types Viral conjunctivitis Bacterial conjunctivitis Chlamydial conjunctivitis Rickettsial conjunctivitis Spiro chaetal conjunctivitis Protozoal conjunctivitis Parasitic conjunctivitis
- 4. BACTERIAL CONJUNCTIVITIS Bacterial conjunctivitis is a common type of pink eye, caused by bacteria that infect the eye through various sources of contamination. The bacteria can be spread through contact with an infected individual, exposure to contaminated surfaces or through other means such as sinus or ear infections.
- 5. BACTERIAL CONJUNCTIVITIS Etiology 1. Predisposing factors Flies, Poor hygienic conditions, Hot dry climate, Poor sanitation and Dirty habits.
- 6. 2. Causative organisms Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus pneumoniae (pneumococcus) , Streptococcus pyogenes (haemolyticus), Haemophilus influenzae (aegyptius, Koch-Weeks bacillus), Moraxella lacunata (Moraxella Axenfeld Bacillus), Pseudomonas pyocyanea, Neisseria gonorrhoeae, Neisseria meningitidis (meningococcus), Corynebacterium diphtheriae.
- 7. 3. According to Mode of infection 1. Exogenous infections may spread: • Directly through close contact, as airborne infections or as waterborne infections • Vector transmission (e.g., flies) • Material transfer such as infected fingers of doctors, nurses, common towels, handkerchiefs, and infected tonometers.
- 8. 2. Local spread may occur from neighbouring structures such as infected lacrimal sac, lids, and nasopharynx. In addition to these, a change in the character of relatively innocuous organisms present in the conjunctival sac itself may cause infections. 3. Endogenous infections may occur very rarely through blood, e.g., gonococcal and meningococcal infections.
- 9. PATHOPHYSIOLOGY Conjuctival discharge Conjuctival tissue response Cellular response Vascular response
- 11. CLINICAL TYPES OF BACTERIAL CONJUNCTIVITIS Acute bacterial conjunctivitis, Hyperacute bacterial conjunctivitis, Chronic bacterial conjunctivitis, and Angular bacterial conjunctivitis.
- 12. ACUTE BACTERIAL CONJUNCTIVITIS Acute bacterial conjunctivitis is characterised by marked conjunctival hyperaemia and mucopurulent discharge from the eye. So, clinically, it is called acute mucopurulent conjunctivitis. It is the most common type of bacterial conjunctivitis.
- 13. CAUSATIVE AGENTS Staphylococcus aureus, Koch-Weeks Bacillus, Pneumococcus and Streptococcus. Mucopurulent conjunctivitis generally accompanies exanthemata such as measles and scarlet fever.
- 14. CLINICAL FEATURES Symptoms Discomfort, foreign body, grittiness, blurring and redness of sudden onset Mild photophobia Mucopurulent discharge from the eyes Sticking together of lid margins with discharge during sleep. Slight blurring of vision due to mucous flakes in front of cornea. Coloured halos Signs Flakes of mucopus Congenctival congestion ‘fiery red eye’ circumcorneal zone congestion Chemosis Fine type Papillae Petechial haemorrhages Cilia with yellow crusts. Eyelids may be slightly oedematous.
- 15. COMPLICATIONS Marginal corneal ulcer Superficial keratitis Blepharitis or dacryocystitis
- 16. TREATMENT Topical antibiotics- broad specturm antibiotics Irrigation of conjunctival sac Dark goggles No steroids should be applied No bandage Anti-inflammatory and analgesic drugs
- 17. ACUTE PURULENT CONJUNCTIVITIS Other names -Hyperacute bacterial conjunctivitis -Acute blenorrhea Clinical picture: Stage of infiltraton Stage of blenorrhoea Stage of slow healing
- 18. HYPERACUTE CONJUNCTIVITIS OF ADULTS (GONOCOCCAL CONJUNCTIVITIS) Etiology The disease affects adults, predominantly males. Gonococcal infection directly spreads from genitals to eye. Presently, incidence of gonococcal conjunctivitis has markedly decreased.
- 19. CLINICAL FEATURE Symptoms Onset is hyper acute (12 to 24 hours) Pain which is moderate to severe Purulent discharge, which is usually copious, Swelling of eyelids, which is usually marked. Signs Tense and swollen eyelids Tenderness Discharge is thick purulent, copius trickling down the cheeks. Chemosis, congestion and papillae, giving bright red velvety appearance. Pseudomembrane appearance conjunctival surface Enlarged and tender preauricular lymph nodes Urethritis and arthritis.
- 20. COMPLICATIONS 1. Corneal involvement - Diffuse haze and oedema, central necrosis, corneal ulceration or even perforation. 2. Iridocyclitis 3. Systemic complications - Gonorrhoea arthritis, endocarditis and septicaemia.
- 21. TREATMENT 1. Systemic therapy Third generation cephalosporin Quinolones Spectinomycin 2. Topical antibiotic therapy 3. Irrigation 4. Other general measures 5. Topical atropine
- 22. CHRO NIC BACTERIAL CONJUNCTIVITIS/ CHRONIC CATARRHAL CONJUNCTIVITIS/ ‘SIMPLE CHRONIC CONJUNCTIVITIS’ A. Predisposing factors 1. Chronic exposure to dust, smoke, and chemical irritants. 2. Local cause of irritation such as trichiasis, concretions, foreign body and seborrhoeic scales. 3. Eye strain due to refractive errors, phorias or convergence insufficiency. 4. Abuse of alcohol, insomnia and metabolic disorders.
- 23. B. Causative organisms Staphylococcus aureus is the commonest cause of chronic bacterial conjunctivitis. Gram negative rods such as Proteus mirabilis, Klebsiella pneumoniae, Escherichia coli and Moraxella lacunata are other rare causes.
- 24. C. Source and mode of infection. 1. As continuation of acute mucopurulent conjunctivitis when untreated or partially treated. 2. As chronic infection from associated chronic dacryocystitis, chronic rhinitis or chronic upper respiratory catarrh. 3. As a mild exogenous infection which results from direct contact, airborne or material transfer of infection.
- 25. CLINICAL FEATURES Symptoms Burning and grittiness in the eyes, especially in the evening. Mild chronic redness in the eyes. Feeling of heat and dryness on the lid margins. Difficulty in keeping the eyes open. Mild mucoid discharge off and on Watering, Feeling of sleepiness and tiredness in the eyes. Signs Grossly the eyes look normal but careful examination may reveal following signs: Congestion of posterior conjunctival vessels. Mild papillary hypertrophy of the palpebral conjunctiva. Sticky look of surface of the conjunctiva. Lid margins may be congested.
- 26. TREATMENT 1. Eliminate predisposing factors when associated. 2. Topical antibiotics such as chloramphenicol, tobramycin or gentamicin should be instilled 3–4 times a day for about 2 weeks to eliminate the mild chronic infection. 3. Astringent eye drops such as zinc-boric acid drops provide symptomatic relief.
- 27. ANGULAR BACTERIAL CONJUNCTIVITIS 1. Predisposing factors are same as for ‘simple chronic conjunctivitis’. 2. Causative organisms Moraxella Axenfield (MA) is the commonest causative organism. MA bacilli are placed end to end, so the disease is also called ‘diplobacillary conjunctivitis’. Rarely, staphylococci may also cause angular conjunctivitis.
- 28. 3. Source of infection - usually nasal cavity. 4. Mode of infection. - Infection is transmitted from nasal cavity to the eyes by contaminated fingers or handkerchief.
- 29. PATHOLOGY The causative organism, i.e., MA bacillus produces a proteolytic enzyme which acts by macerating the epithelium. This proteolytic enzyme collects at the angles by the action of tears and thus macerates the epithelium of the conjunctiva, lid margin and the skin, the surrounding angles of eye. The maceration is followed by vascular and cellular responses in the form of mild grade chronic inflammation. Skin may show eczematous changes.
- 30. CLINICAL FEATURES Symptoms Irritation Burning sensation and feeling of discomfort in the eyes History of collection of dirty-white foamy discharge at the angles Redness in the angles of eyes. Signs Hyperaemia of bulbar conjunctiva near the canthi. Hyperaemia of lid margins near the angles Excoriation of the skin around the angles. Foamy mucopurulent discharge at the angles is usually present.
- 31. COMPLICATIONS Blepharitis and Shallow marginal catarrhal corneal ulceration.
- 32. TREATMENT A. Prophylaxis includes treatment of associated nasal infection and good personal hygiene. B. Curative treatment consists of: 1. Oxytetracycline (1%) eye ointment, 2–3 times a day for 9–14 days will eradicate the infection. 2. Zinc lotion instilled in day time and zinc oxide ointment at bed time inhibits the proteolytic ferment and thus helps in reducing the maceration.
- 33. THANK YOU