Download to read offline
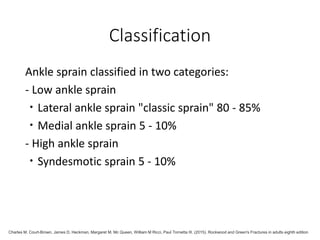
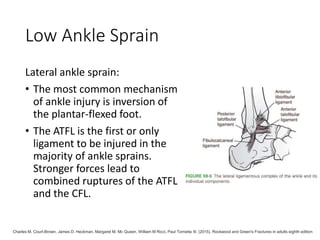


- Ankle sprains are the most common type of ankle injury, with lateral ankle sprains making up 80-85% of cases. Inversion injuries are most common. - Chronic ankle instability affects 20-40% of patients with a previous ankle sprain. The ATFL ligament is most frequently injured. - Ankle sprains are classified as low (lateral or medial) or high (syndesmotic). A lateral sprain typically injures the ATFL ligament. - Conservative treatment involves RICE (rest, ice, compression, and elevation) and rehabilitation. Surgical reconstruction may be needed for grade III injuries or recurrent instability.



































































