Spermiogenesis or Spermateleosis or metamorphosis of spermatid
Renal system bundle.pdf
1. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
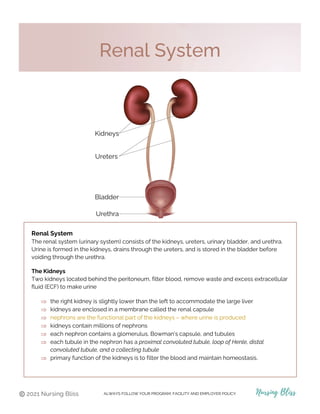
Renal System
The renal system (urinary system) consists of the kidneys, ureters, urinary bladder, and urethra.
Urine is formed in the kidneys, drains through the ureters, and is stored in the bladder before
voiding through the urethra.
The Kidneys
Two kidneys located behind the peritoneum, filter blood, remove waste and excess extracellular
fluid (ECF) to make urine
⇒ the right kidney is slightly lower than the left to accommodate the large liver
⇒ kidneys are enclosed in a membrane called the renal capsule
⇒ nephrons are the functional part of the kidneys – where urine is produced
⇒ kidneys contain millions of nephrons
⇒ each nephron contains a glomerulus, Bowman’s capsule, and tubules
⇒ each tubule in the nephron has a proximal convoluted tubule, loop of Henle, distal
convoluted tubule, and a collecting tubule
⇒ primary function of the kidneys is to filter the blood and maintain homeostasis.
Renal System
2. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Urine Formation & Excretion
⇒ urine is continually formed in the kidneys
⇒ fluid flows through the tubules and water and electrolytes, are reabsorbed or secreted;
waste is excreted
⇒ urine drains from the collecting ducts of nephrons into the calix
⇒ the calices (plural of calix) drain into the renal pelvis
⇒ urine drains from the renal pelvis of each kidney into the ureter to be stored in the bladder
then exits the body through the urethra
⇒ proteins and blood cells do not pass into the tubules
Renal System
3. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
renal capsule – protective, fibrous outer layer of the kidneys
renal cortex – outer layer inside the capsule of the kidney; contains glomerulus and bowman’s
capsule, renal tubules
renal medulla – inner area containing the renal pyramids and renal tubules
nephrons – composed of glomerulus, Bowman’s capsule, and tubules; secretes and reabsorbs
fluid, electrolytes, acids, and bases; excretes waste
glomerulus – surrounded by Bowman’s capsule; blood enters under high pressure for
ultrafiltration and produces filtrate
tubules – located in both the cortex and medulla where reabsorption and secretion of most
water, electrolytes, glucose, acids, bases takes place
loop of Henle – reabsorbs water, sodium, and chloride; helps maintain fluid and sodium
balance
Renal System
4. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Renal System
Glomerular filtration rate (GFR)
• amount of blood filtered each minute by the glomeruli
• normal GFR is 90 – 120 mL/min; it decreases with age
Labs to Know
BUN 7-20 mg/dL
Creatinine 0.6-1.2 mg/dL
Specific Gravity 1.010-1.030
GFR 90-120 mL/min
Functions of the Kidneys
• excrete waste products from the body
• excrete toxins, water-soluble medications
• maintain acid-base balance
• control fluid and electrolyte balance
• secrete renin to regulate blood pressure
• secrete erythropoietin to stimulate bone marrow to produce red blood cells
• convert vitamin D to an active form for calcium absorption and regulation
• this process results in the formation of urine
Blood Supply to the Kidneys
renal artery – oxygenated blood flows from the heart to the kidneys to be filtered. Blood flows
into the capillaries of the glomerulus from the afferent arteriole.
renal vein – filtered blood from the efferent arterioles in the kidneys flows back to the heart for
oxygenation. Blood flows out of the capillaries of the glomerulus from the efferent arteriole.
5. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Renal System
Anatomy of a Nephron
Renal Corpuscle <
glomerulus & Bowman’s capsule
renal tubule
proximal convoluted tubule (PCT)
loop of Henle
distal convoluted tubule (DCT)
collecting tubule (aka collecting
duct)
Regulation of Blood Pressure
RAAS
The renin-angiotensin-aldosterone system is essential
for the regulation of blood pressure and fluid balance.
*See homeostasis of sodium for pathophysiology
and the illustration on the next page.
6. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Renal System - Homeostasis
Homeostasis of Water
• Antidiuretic hormone (ADH) is essential for reabsorption of water in the kidneys
• without ADH water cannot pass through the tubules and will be voided
• secretion of ADH by the pituitary gland is stimulated by ↑sodium intake, dehydration and
by ↓blood volume
• water is drawn out of the tubules by osmosis and goes back into the blood
• a person that does not produce enough ADH develops diabetes insipidus (DI)
• DI patients cannot survive without treatment because they will void too much dilute urine
to survive
RAAS System
7. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Renal System - Homeostasis
Homeostasis of Potassium
• increased potassium levels stimulate the release of aldosterone
• aldosterone stimulates the tubules to secrete potassium
• potassium levels return to normal
↑potassium (K+)→ release of aldosterone→ tubules secrete potassium (K+)→ potassium (K+)
returns to normal levels
Homeostasis of Sodium
• when sodium intake is increased, water is retained by the body to maintain osmotic
pressure
• increased sodium means an increase in blood volume and BP
• filtration in the glomerulus increases, secreting water and sodium to return BP to normal
↑sodium → ↑blood pressure→ ↑ glomerulus filtration→ ↑water, sodium excretion →normal BP
• the renin-angiotensin-aldosterone system (RAAS) controls the reabsorption of
sodium
• when the BP or sodium is low, an enzyme called renin is released from the
juxtaglomerular cells in the kidneys
• renin activates angiotensinogen (from the liver) to angiotensin I
• angiotensin I is converted to angiotensin II by angiotensin-converting enzyme (ACE) in the
lungs
• angiotensin II (potent vasoconstrictor) stimulates the release of aldosterone
• tubules (DCT) reabsorb sodium and secrete potassium
• sodium increases water reabsorption and blood volume; BP returns to normal
• renin stops being secreted
↓BP or sodium→ renin released→angiotensinogen→angiotensin I→ angiotensin II by ACE→ ACE
stimulates aldosterone release→ tubules reabsorb NA+, secrete K+ → normal BP→renin stops
8. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Urinary Tract Infections
Urinary tract infections (UTIs) are infections of the urinary tract. They are the most common
bacterial infection in women.
⇒ Escherichia coli (E. coli) is the most common bacteria causing a UTI
⇒ catheter associated urinary tract infections (CAUTIs) are often caused by E. coli
⇒ bacterial UTIs can involve the urethra, bladder, kidneys; prostate in men
⇒ may be asymptomatic or include painful urination, urgency, and frequency
⇒ diagnosis is by urinalysis and sometimes urine culture
⇒ UTIs are the most common healthcare-associated (HAI) infection; primarily from use of
indwelling catheter
⇒ classified as upper or lower UTI, but sometimes it is impossible to distinguish
Urinary Tract Infections
9. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Urinary Tract Infections
urethritis is an inflammation of the urethra. In men the most common cause is by a sexually
transmitted infection. In women it is commonly caused by irritants, such as scented toilet paper,
sanitary napkins, spermicide, or also by a UTI.
cystitis is an inflammation of the bladder caused by an infection, irritant, or obstruction of the
urethra
pyelonephritis is inflammation of the renal pelvis and the parenchyma (functional part of kidney)
caused by bacterial infection. Acute pyelonephritis can occur following an invasive procedure of
the urinary tract
Urosepsis is a UTI that has spread systemically. It is a medical emergency and can lead to septic
shock and death. Bacteriuria (bacteria in urine) and bacteremia (bacteria in blood) is a sign of
urosepsis
Pathophysiology
Urine maintains an antibacterial characteristic by an acidic pH (less than 6.0), high urea
concentration, and glycoproteins that inhibit the growth of bacteria.
The organisms that usually cause UTIs originate in the perineum (area between the anus and
scrotum or vulva) and are introduced through the urethra and ascend upward toward the bladder.
Uncomplicated UTIs occur in a normal urinary tract and usually involve the bladder only.
Complicated UTIs occur in a person with a problem in the urinary tract such as stones, catheter,
acute kidney injury, chronic kidney disease; or in diabetes, or pregnancy-induced changes, etc.
Urinary Tract Infections
10. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Cystitis is an inflammation of the bladder caused by an infection, irritant, or obstruction of the
urethra.
⇒ more common in women because the urethra is shorter than in men and in women it is
located near the rectum
⇒ sexually active and pregnant women are more vulnerable to cystitis
Diagnosis
• dipstick urinalysis
• urinalysis (clean-catch, mid-stream)
• urine culture (in recurrent UTIs)
Nursing Interventions
• Before admin of prescribed antibiotics, obtain urine specimen for culture if prescribed
• encourage fluids 3000 mL/day
• maintain an acid urine pH (5.5)
• sterile technique is mandatory when inserting a catheter
• maintain catheter, manage fluid intake, prevent infection
• discourage coffee, colas
• acidic urine decreases the actions of aminoglycosides, sulfonamides, and nitrofurantoin
Cystitis
Causes
• irritants – soaps, scented toilet paper
& sanitary napkins
• calculus (stones)
• indwelling catheter
• sexual intercourse
• spermicides
• urinary stasis
• synthetic underwear
• wet bathing suit
Signs & Symptoms
• painful, burning urination
• frequency and urgency
• voiding small amounts
• incomplete or inability to empty bladder
• cloudy, dark urine, foul smell
• blood in the urine
• WBC > 11,000 mm3, urinalysis
The elderly often present with mental
confusion.
11. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Cystitis
Upper & Lower UTI Signs & Symptoms
Patient Education
• avoid alcohol, caffeine, citrus
• consume foods to maintain acidic urine (cranberry
juice)
• take antibiotics as prescribed and complete entire
course
• follow-up urine culture after treatment
teach prevention of recurrence of cystitis
• wipe front to back
• void every 2 – 3 hours
• if pregnant, void every 2 hours
• avoid synthetic underwear and tight clothes
• avoid bubble baths
Treatment
• fluids
• antibiotics, analgesics
• removal of urinary
catheter if present
Medications
• antibiotics
• analgesics
• antimicrobials
• antiseptics
• antispasmodics
Upper UTI
pyelonephritis
Signs & Symptoms
• fever, chills
• flank pain
• nausea, vomiting
• headache
• malaise
• dysuria
• bacteriuria (bacteria in urine) and
bacteremia (bacteria in blood) is a sign
of urosepsis
Lower UTI
urethritis, cystitis
Signs & Symptoms
• painful, burning urination
• frequency and urgency
• voiding small amounts
• incomplete or inability to empty bladder
• cloudy, dark urine, foul smell
• blood in the urine
• WBC > 11,000 mm3, urinalysis
Elderly often present with mental confusion.
12. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Pyelonephritis
Signs & Symptoms
• fever, chills
• flank pain
• nausea, vomiting
• headache
• malaise
• dysuria
• bacteriuria (bacteria in urine) and bacteremia
(bacteria in blood) is a sign of urosepsis
Pyelonephritis (Kidney Infection)
is Inflammation of one or both kidneys caused by a bacterial infection.
⇒ can be acute or chronic
⇒ acute pyelonephritis most commonly occurs after a bacterial infection of the urethra
⇒ the infection ascends the urinary tract to the kidneys
⇒ can progress to chronic pyelonephritis
⇒ chronic pyelonephritis occurs with urinary flow obstruction with reflux into the renal pelvis
⇒ slow, progressive disease
⇒ can lead to acute kidney injury (AKI) or chronic kidney disease (CKD)
⇒ CAUTI is a common cause of pyelonephritis for residents of long-term care facilities
• Diagnosis
• urinalysis
• urine culture
• ultrasound
• CT scan
Nursing Interventions
Monitor
• temperature
• I & O, weight (output minimum of 1500 mL / 24
hours)
• for signs of AKI or CKD
• encourage fluids to 3000 mL/day
• admin pain meds, antibiotics, antipyretics, antiemetics
as prescribed
Patient Education
• educate on high-calorie, low-protein diet
• encourage follow up urine culture
Signs of AKI
• oliguria
• hyperkalemia
• hematuria
Signs of CKD
• confusion
• HTN
• hypervolemia (fluid
volume) excess
13. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Terms to Know
NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Terms to Know
frequency – increased incidence of urination
urgency – voiding more than every 2 hours
incontinence -involuntary urination
dysuria – painful or difficult urination
nocturia – frequent urination at night
hematuria – blood in the urine
proteinuria – protein in the urine
pyuria – pus in the urine
polyuria – large volume of urine in a period of time
enuresis – involuntary nocturnal urination
oliguria – production of abnormally small amounts of urine
anuria – <100 mL/24 hours
bacteriuria - bacteria in the urine
bacteremia - bacteria in the blood
14. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Causes & Risk Factors
• diabetes
• hypertension
• immune disease (e.g., Goodpasture syndrome, scleroderma)
• viral infections (hepatitis B, C, HIV)
• group A beta-hemolytic streptococcal infection (strep throat, or impetigo)
• history of sore throat 1 – 2 weeks before symptoms
Complications
• kidney failure
• pulmonary edema
• heart failure
• hypertensive encephalopathy
• seizures
Glomerulonephritis (GN) is inflammation of the glomeruli. It refers to a group of kidney disorders
that cause inflammatory injury in the kidneys.
⇒ glomerulonephritis affects both kidneys equally
⇒ destruction of the glomeruli in the kidneys
⇒ ↓ GFR (glomerular filtration rate)
⇒ temporary or permanent loss of kidney function can occur
⇒ can be asymptomatic (hematuria or edema around the eyes often the first symptom)
Types
acute glomerulonephritis comes on suddenly and is reversable. Occurs 1 – 2 weeks after a
streptococcal infection
chronic glomerulonephritis can occur after the acute phase or slowly over time and can lead to
permanent renal failure
Glomerulonephritis
15. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Acute Poststreptococcal Glomerulonephritis
⇒ a common type of acute glomerulonephritis
⇒ most common in children, and older adults
⇒ most cases resolve completely
⇒ develops after strep throat or impetigo
⇒ a normal functioning glomerulus filters water, electrolytes, and waste from the blood, but
does not allow blood cells and proteins to pass into the tubules because blood cells and
proteins are too large
Pathophysiology
⇒ the person with strep throat makes antibodies to the streptococcal antigen and these
antibodies reach the glomerulus and cause inflammation and damage allowing proteins and
red blood cells to permeate the glomerulus
⇒ the protein and blood cells pass into the urine
⇒ the exact way the tissue in the glomerulus is damaged is not known
Acute Glomerulonephritis
Signs & Symptoms
• hematuria (cloudy, dark brown urine)
• proteinuria (protein present, foamy
urine)
• hypertension
• edema around the eyes
• decreased urinary output
• oliguria
• ↑blood urea nitrogen (BUN)
• ↑creatinine levels
Diagnosis
• urinalysis
• serum creatinine
• blood urea nitrogen (BUN)
17. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Nephrotic Syndrome
Nephrotic Syndrome (NS)
Nephrotic syndrome results when the glomerulus is excessively permeable to protein.
This causes massive proteinuria, low plasma albumin and tissue edema.
⇒ more common in children but can occur at any age
⇒ urinary protein ≥3 g/24 hours confirms diagnosis
⇒ ↑risk for infection
⇒ ↑risk for blood clots
⇒ hypocalcemia may occur
Pathophysiology
⇒ the increased permeability of the glomerular membrane allows for massive leakage of
protein in the urine >3 g/24 hours
⇒ this results in decreased protein in the blood and decreased oncotic pressure → edema
⇒ ascites and massive generalized edema will develop if there is severe hypoalbuminemia
⇒ ↓albumin stimulates the liver to produce more albumin and lipids → high cholesterol and
triglycerides in patient
Signs & Symptoms
• edema
• massive proteinuria
• hypoalbuminemia
• hyperlipidemia
• foamy urine
Diagnosis
• proteinuria ≥3 g/24 hours
• edema
• renal biopsy if cause is unknown
Primary Causes
• minimal change disease (in children)
• focal segmental glomerulosclerosis
• acute glomerulonephritis
• rapidly progressive
glomerulonephritis
Secondary Causes
• infections
• Lupus
• Diabetes
19. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Terms to Know
NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Terms to Know
frequency – increased incidence of urination
urgency – voiding more than every 2 hours
incontinence -involuntary urination
dysuria – painful or difficult urination
nocturia – frequent urination at night
hematuria – blood in the urine
proteinuria – protein in the urine
pyuria – pus in the urine
polyuria – large volume of urine in a period of time
enuresis – involuntary nocturnal urination
oliguria – production of abnormally small amounts of urine
anuria – <100 mL/24 hours
bacteriuria - bacteria in the urine
bacteremia - bacteria in the blood
20. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Renal Calculi
are stones that can form anywhere in the urinary tract
⇒ also known as kidney stones and nephrolithiasis
⇒ can form in the kidneys, ureters, bladder
⇒ they are most common in the kidneys
⇒ can be as small as a grain of sand, size of a pea or as large as a golf ball
⇒ calculi can cause obstruction, trauma to tissue (w/bleeding), infection, and severe pain
⇒ when a stone obstructs a ureter and blocks the flow of urine hydroureter can develop
⇒ urinary stasis (urine stationary in tract) ↑risk for more stones, infection, hydronephrosis,
permanent kidney damage
⇒ after the stone is passed, analysis is done to determine the type of stone and treatment
⇒ types of stones are calcium oxalate, calcium phosphate, uric acid, cystine, and struvite
Pathophysiology
dehydration, immobility, or another contributing factor → crystalized minerals and salts form in
the filtrate of the nephrons → minerals and salts in supersaturated urine stick together to form a
stone
Renal Calculi
21. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Causes & Risk Factors
• family history of renal stones
• immobility
• gout (↑uric acid level)
• UTIs
• urinary catheter extended use
• obstruction → urinary stasis
• dehydration (↑ solute concentration)
• warm climate
• low fluid intake
• diuretics
• diet
• excess tea, fruit juices ↑oxalate
• high protein ↑uric acid
• high in salt
• GI problems
calculus - stone
nephrolithiasis - kidney stones (nephro – kidney, lithiasis – stone formation)
urolithiasis – stones form in the ureter
renal cholic – sharp, severe pain in the flank area, lower back or lower abdomen caused by
stretching, dilation and spasm of the ureter by the stone
hydronephrosis – enlargement of the renal pelvis and calyces.
Renal Calculi
Complications
• obstruction of urine flow
• hydronephrosis
• hydroureter
• infection
• renal failure
Diagnosis
• urinalysis
• CT scan or ultrasound
22. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Signs & Symptoms
• renal colic – stone in renal pelvis (severe, pain that radiates from costovertebral area or
the flank down to the genital area)
• ureteral colic – stone in ureter (severe, sharp pain radiating along the area of the ureter to
the genital area)
• nausea, vomiting
• diaphoresis (sweating)
• hematuria
• signs of a UTI
• fever, chills
• WBC & RBC in urine
Nursing Interventions
• pain management
• ↑fluids up to 3000 mL/day
• strain ALL urine for stones and send to
the lab
(to dx underlying problem & treat pt.)
• heat to the flank area (NO massage)
• admin pain medication as scheduled (not
PRN)
• encourage ambulation (turn immobile
patient)
Monitor
• intake and output
• for fever, infection
• for obstruction
Renal Calculi
Patient Education
• stones can reoccur
• ↑fluid (water) intake to about 3
L/day to prevent recurrence
• low sodium diet
• may have diet restrictions based
on the stone type
Diet Restrictions Based on Stone Type
Uric acid stones – avoid purine-rich foods: alcohol, organ
meats, red meat, sardines
Calcium oxalate stones – avoid oxalate-rich foods:
spinach, rhubarb, beets, cabbage tomatoes, nuts, sweet
potatoes, chocolate, tea
23. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Renal Calculi
Medications
• NSAIDs if not contraindicated
• Opioids
Treatment
Non-invasive
extracorporeal shock-wave lithotripsy (ESWL)
• shock waves shatter the stone into smaller pieces
• patient must increase fluids to flush out stone fragments
Invasive
ureteroscopy
• scope inserted through urethra to the area of the stone and uses laser lithotripsy to
break up the stone
percutaneous nephrolithotomy
• incision is made in the back to insert nephroscope into kidney
• a laser may be used to break larger stones into smaller fragments
• patient must increase fluids to flush out stone fragments
24. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Benign Prostate Hyperplasia (BPH) is a condition in which the prostate gland slowly enlarges
and obstructs the urethra
⇒ common condition in men over 50 and increases with age
⇒ disrupts outflow of urine from the bladder
⇒ can progress to complete obstruction
⇒ have lower urinary tract symptoms (LUTS)
⇒ BPH does not cause or increase risk for prostate cancer
hyperplasia – increase in production rate of cell growth
hypertrophy – increase in size of cells
Pathophysiology
as men age hormonal changes may stimulate prostate cell growth → progressive enlargement
of the prostate → narrowing of the urethra → urine outflow increasingly restricted
Benign Prostatic Hyperplasia
25. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Signs & Symptoms
• weak stream
• urgency
• frequency
• hesitancy (inability to start stream)
• dribbling
• incomplete bladder emptying
• urinary stasis
• UTIs
• hematuria
Causes
Not completely understood
• hormonal changes with aging
• genetics
Benign Prostatic Hyperplasia
Risk Factors
• aging
• obesity
• sedentary lifestyle
• family history
Complications
• Complications are rare
• chronic urinary retention
• UTIs
• bladder stones
Diagnosis
• clinical symptoms
• rectal exam
• urinalysis
Nursing Interventions
• encourage fluids 2000 – 3000 mL/day
unless contraindicated
• urinary catheterization
• admin meds to
o shrink prostate gland
o relax prostate smooth muscle
• avoid admin meds that cause urinary
retention
o antidepressants
o anticholinergics
o antihistamines
o decongestants
Treatment
• medications
• transurethral resection of the prostate
(TURP)*
*Removal of prostate tissue using a
resectoscope that is inserted through the
urethra
Medications
• 5α-reductase inhibitors (shrink prostate)
• α-adrenergic receptor blockers (relax
smooth muscle)
Patient Education
• limit caffeine, spicy foods
• bladder retraining (voiding schedule)
26. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Acute Kidney Injury (Kidney Failure)
acute kidney injury (AKI) is the sudden loss of kidney function
⇒ often follows exposure to a nephrotoxin, prolonged hypotension, or hypovolemia
⇒ AKI can be reversable but has a high mortality rate
⇒ prognosis depends on the cause and the condition of the patient
⇒ causes are complex and classified as prerenal, intrarenal, and postrenal
⇒ prerenal and postrenal AKI that has not caused kidney damage usually resolves quickly
with treatment
⇒ there are 4 phases of AKI: onset, oliguric, diuretic, recovery
⇒ fluid, electrolyte, and acid-base imbalance develops quickly
⇒ when a patient does not recover from AKI, chronic kidney disease (CKD) may develop
⇒ infection is the leading cause of death in AKI (elevated temp is NOT always present)
Acute Kidney Injury
27. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Causes and Pathophysiology
Prerenal – outside the kidney
↓renal blood flow → reduced glomerular perfusion and filtration of the kidneys
• hemorrhage
• dehydration, diarrhea, vomiting
• ↓cardiac output
• obstruction (prerenal)
• infection (prerenal)
Intrarenal – within the kidney
direct damage to the kidney → impaired nephron function
• prolonged ischemia
• nephrotoxins (NSAIDs, contrast dye)
• acute tubular necrosis (ATN)
• obstruction (intrarenal)
• infections (intrarenal)
Postrenal – after the kidney (ureters, bladder, or urethra)
involves obstruction of the outflow of urine → urine reflux into the renal pelvis → impaired
kidney function
• benign prostatic hyperplasia (BPH)
• prostate cancer
• bladder cancer
• stones
• infections (postrenal)
Acute Kidney Injury
28. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Signs & Symptoms
Signs and symptoms of AKI are caused by retention of urea nitrogen, creatinine, fluids, and the
kidneys unable to regulate electrolytes.
Onset Phase
event causes injury → symptoms
Acute Kidney Injury
• fluid volume overload
edema
hypertension
dysrhythmias
heart failure
pulmonary edema
pericardial and pleural effusions
• metabolic acidosis
Kussmaul’s respirations (rapid, deep
inspirations)
• hyperkalemia
• uremia
anorexia
nausea, vomiting
• pericarditis
chest pain with inspiration
low-grade fever
• neurologic changes
fatigue
seizure
coma
Treatment
• dialysis
Diuretic Phase
• urine output gradually increases
• then osmotic diuresis occurs (high urea
concentration in the filtrate) 4 – 6 L/day
• risk of hypovolemia, hypotension
• risk of hypokalemia, hyponatremia
• 1 – 3 weeks duration
Recovery Phase
• begins when GFR increases
• serum BUN and creatinine decrease
• urine volume normal
• can take a year or more to recover
• older adult may not fully recover
• can progress to CKD (chronic kidney
disease) or ESRD (end stage renal
Oliguric Phase
sudden onset oliguria is the most common initial manifestation
• duration 10-14 days (the longer the oliguric phase = the poorer the prognosis)
• sudden oliguria, <400 mL/day output (some pts. have >400 mL/day
29. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Acute Kidney Injury
Nursing Interventions
Monitor
• daily weights (same scale, same time of day)
• vital signs
• strict intake & output
• urine color, specific gravity, protein, glucose, blood, casts
• for signs of infection
• auscultate lungs for crackles, wheezes, ↓breath sounds
• edema, neck vein distention
• heart for tachycardia, irregular HR, pericardial friction rub
• BUN, creatinine, electrolytes
• LOC
• dialysis access site for exudate
• prepare patient for dialysis if prescribed
• admin medications as prescribed
• ↓potassium diet as prescribed
Medications
• diuretics
• calcium gluconate IV
• insulin IV
• glucose IV
• Kayexalate (contraindicated w/ paralytic ileus)
• sodium bicarbonate
Diagnosis
• creatinine & creatinine clearance
• GFR (glomerular filtration rate)
• BUN (blood urine nitrogen)
• serum electrolytes
• urinalysis
• renal scan or ultrasound
Normal Lab Values
creatinine level 0,6 – 1.20 mg/dL
creatinine clearance
85 – 125 mL/min (female)
95 – 140 mL/min (male)
GFR ≥90 mL/min
30. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Chronic Kidney Disease
a progressive, irreversible loss of kidney function
⇒ as kidney function worsens CKD affects all body systems
⇒ CKD defined as a GFR ≤60 mL / minute for 3 months or more
⇒ CKD is more common than AKI (acute kidney injury)
⇒ occurs in 5 stages and results in end-stage renal disease (ESRD)
⇒ kidneys are unable to excrete enough sodium and water; hypervolemia results
⇒ some can live normal lives with CKD, while others progress rapidly to ESRD
Pathophysiology
At first a gradual loss of nephrons is unnoticeable because the kidneys adapt with the normal
tissue increasing its function → kidney function decreases to the point that healthy nephrons can
no longer increase their function → urea, creatinine, phenols, hormones, electrolytes, and water
are retained → uremia develops → ESRD
uremia – a syndrome with raised levels of urea in the blood to the point where symptoms
develop in multiple body systems.
Chronic Kidney Disease
Causes
• diabetes
• acute kidney injury
• hypertension
• chronic urinary obstruction
• recurring infections
• polycystic disease
• autoimmune disorders
• nephrotoxic drugs (e.g., NSAIDS, contrast dyes,
aminoglycoside antibiotics)
Risk Factors
• diabetes
• hypertension
• CVD (cardiovascular disease)
• >60 years old
• black or Native American
• family hx of CKD
31. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Stages
GFR decreases with progression of CKD
Stage 1
Normal renal function >90 mL/min
(proteinuria for ≥3 months
Stage 2
Mild CKD 60-80 mL/min
Stage 3
Moderate CKD 30-59 mL/min
Chronic Kidney Disease
Stage 4
Severe CKD 15-29 mL/min
Stage 5
ESRD <15 mL/min
Signs & Symptoms
As kidney function worsens, CKD affects all body systems. Symptoms almost always present are:
• anorexia
• nausea
• vomiting
• weight loss
• unpleasant, metallic taste in mouth
Physiologic
• anxiety
• depression
Neurologic
• lethargy
• tremors
• coma
Cardiovascular
• hypertension
• heart failure
• coronary artery disease
• pericarditis
• peripheral edema
Respiratory
• crackles, SOB
• Kussmal’s respirations
• pulmonary edema
Hematologic
• bleeding, bruising
• anemia
Gastrointestinal
• anorexia, nausea,
vomiting
• GI bleeding
• gastritis
Renal/Urinary
• polyuria (early sign)
• oliguria (late sign)
• proteinuria
• hematuria
Musculoskeletal
• muscle weakness
• muscle cramping
• bone pain
Integumentary
• pruritis
• ecchymosis
• poor skin turgor
• uremic frost (late sign)
Reproductive
• absent menses
• erectile dysfunction
32. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
CKD ↑ Risk of:
• anemia
• GI Bleeding
• hypertension
• infection
• metabolic acidosis
Chronic Kidney Disease
Nursing Interventions
(The same interventions as for AKI)
Monitor
• daily weights (same scale, same time of day)
• vital signs
• strict intake & output
• urine color, specific gravity, protein, glucose, blood, casts
• for signs of infection
• auscultate lungs for crackles, wheezes, ↓breath sounds
• edema, neck vein distention
• heart for tachycardia, irregular HR, pericardial friction rub
• BUN, creatinine, electrolytes
• LOC
• dialysis access site for exudate
• prepare patient for dialysis if prescribed
• admin medications as prescribed
Patient Education
• diet restrictions – sodium, potassium, phosphate
• fluid restrictions
• S/s of electrolyte imbalance, especially high
potassium
• daily weights
Treatment
• ACE inhibitors
• ARBs
• erythropoietin-stimulating agents
• lipid lowering medications
Renal Replacement Therapy (RRT)
• dialysis
• kidney transplant
33. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
AKI CKD
ONSET SUDDEN
GRADUAL – OVER MANY
YEARS
COMMON CAUSE ACUTE TUBULAR NECROSIS DIABETIC NEPHROPATHY
DIAGNOSIS
SUDDEN REDUCTION IN URINE
OUTPUT AND/OR ↑CREATINE
GFR <60 ML/MIN, >3 MONTHS
REVERSIBLE? POSSIBLE NO, PROGRESSIVE
PRIMARY CAUSE OF
DEATH
INFECTION CARDIOVASCULAR DISEASE
AKI & CKD Comparison
Acute Kidney Injury & Chronic Kidney Disease
34. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Dialysis
the movement of fluid and particles across a semipermeable membrane from one compartment
to another
Two types available: Hemodialysis (HD) Peritoneal Dialysis (PD)
Hemodialysis (HD)
renal replacement therapy using a dialyzer with an artificial semipermeable membrane, usually
cellulose-based
⇒ diffusion of particles move from the blood through a semipermeable membrane and into
a dialysis solution (dialysate)
⇒ proteins and RBCs are too large to pass through the membrane
⇒ removes waste from the blood
⇒ corrects fluid and electrolyte imbalances
⇒ the nephrologist determines when to start dialysis based on the patients’ clinical status
(not just the GFR)
⇒ can be used to treat drug overdose
Dialysis
Hemodialysis
35. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Requires Vascular Access
• arteriovenous fistula (AVF)
o connects an artery to a vein
o placed 3 months before starting HD
o feel the thrill (palpate →buzzing sensation)
o hear a bruit (rushing sound w/stethoscope)
• arteriovenous graft (AVG)
o made of synthetic material placed between artery & vein
o needs 2-4 weeks to heal before dialysis
o prone to infection & clots more than AVF
• both require surgery
Hemodialysis
Nursing Interventions
• weigh patient before and after HD
Assess for:
• patency of AVF or AVG before, during, after
• fluid volume hyper-, hypo- before and after
Monitor
• vitals
• for high temperature
• BUN, creatinine, CBC before, during, after
• for bleeding
NO BP, IVs, blood draws in arm with AV fistula or graft
Hospitalized patient – label with armband with No BPs, IVs, blood draws, in this arm
Complications of HD
• hypotension
• dialysis disequilibrium syndrome
• hemolysis (rupture of red blood
cells)
• air embolism (foam in venous blood
line of dialyzer)
• electrolyte imbalance
• sepsis
• shock
36. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Peritoneal Dialysis
Peritoneal dialysis (PD)
the peritoneal membrane (abdominal) acts as the semipermeable membrane
⇒ access is through a peritoneal catheter
⇒ 3-5 cm below umbilicus
⇒ PD is done by putting dialysis solution into the peritoneal space
⇒ it is critical to maintain an aseptic technique to avoid peritonitis
⇒ can be done bedside or at home by patient
⇒ all dialysis solutions are prescribed by the PHCP
⇒ the higher the glucose concentration the more fluid removed during PD exchange
Contraindicated in patients with
⇒ peritonitis
⇒ recent abdominal surgery
⇒ other GI problems
37. ALWAYS FOLLOW YOUR PROGRAM, FACILITY AND EMPLOYER POLICY.
Nursing Interventions
• weigh patient before and after PD
Before PD Assess
• catheter site
• electrolyte & glucose levels
• fluid volume ↑↓before and after
During PD Monitor
• vitals
• BP
• for bleeding at site
• pulmonary edema
• dwell time – do not exceed PHCP’s prescription, ↑risk hyperglycemia
• outflow for color, clarity
• notify PHCP if outflow is cloudy – may indicate infection
Peritoneal Dialysis
Types of PD
Automated peritoneal dialysis (APD)
• most popular because patients do at home
while they sleep
Continuous ambulatory peritoneal dialysis (CAPD)
• done every few hours during the day
Three Phases of a PD Cycle
• inflow (fill)
• dwell (equilibration)
• drain
the 3 phases are one exchange
Complications of PD
• infection of catheter site
• peritonitis
• abdominal pain
• leakage at catheter site
• insufficient outflow
• bleeding
• protein loss