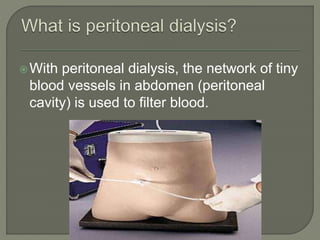
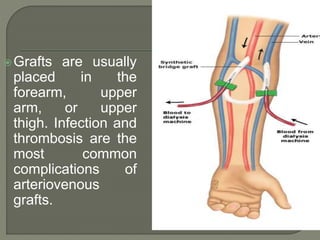
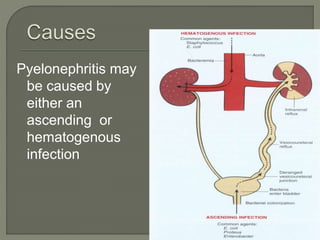
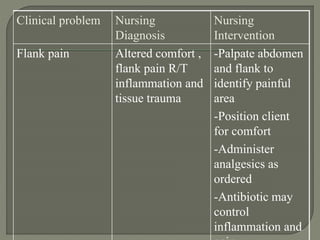
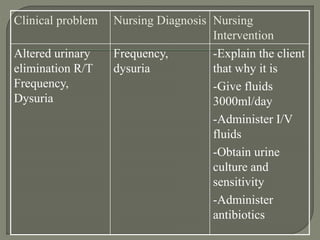
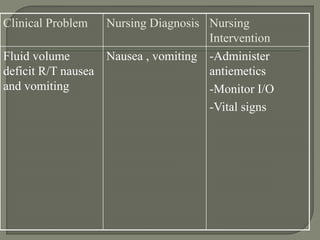
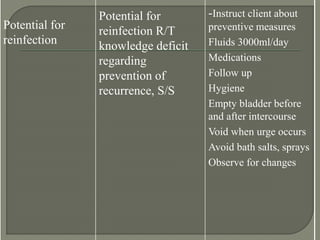
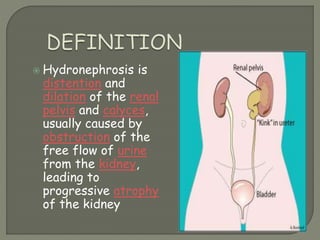
The document discusses pyelonephritis, which is an inflammation of the renal pelvis and parenchyma caused by a bacterial infection. It can be caused by an ascending or hematogenous infection. Symptoms include flank pain, fever, vomiting and frequent urination. Diagnosis involves urine culture and sensitivity as well as imaging tests. Treatment aims to eliminate pathogenic organisms with antibiotics based on culture results and remove any contributing factors to decreased resistance. Mild cases may only require a short course of oral antibiotics while severe cases involving abscesses may require IV antibiotics or even drainage of abscesses.




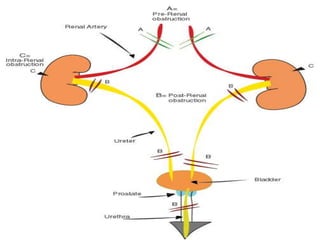
























![ It depend upon
whether the
obstruction is
acute or chronic,
partial or complete,
unilateral or bilateral.
Unilateral
hydronephrosis may
occur without any
symptoms, while acute
obstruction can cause
intense pain.[1]](https://image.slidesharecdn.com/finalrenalseminar-220922051029-1b2b123a/85/final-renal-seminar-pptx-394-320.jpg)