Respiratory arrest and inssufficiency
•
13 likes•11,627 views

OM VERMA ASSISTANT PROFESSOR GRACIOUS COLLEGE OF NURSING( C.G)

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Respiratory arrest and inssufficiency
Similar to Respiratory arrest and inssufficiency (20)
More from OM VERMA
More from OM VERMA (20)
Recently uploaded
Recently uploaded (20)
Respiratory arrest and inssufficiency
- 1. RESPIRATORY FAILURE AND INSUFFICIENCY PRESENTED : MR.OM VERMA ASSISTANT PROFESSOR RELIANCE INSTITUTE OF NURSING
- 3. INTRODUCTION RESPIRATORY FAILURE ( AREEST) results from inadequate gas exchange by the respiratory system, meaning that the arterial oxygen, carbon dioxide or both cannot be kept at normal levels. A drop in the oxygen carried in blood is known as hypoxemia; a rise in arterial carbon dioxide levels is called hypercapnia. INSUFFICIENCY the quality or state of not being sufficient: as. a : lack of adequate supply of something an insufficiency of vitamins. b : lack of physical power or capacity especially inability of an organ or bodily part to function normally renal insufficiency pulmonary insufficiency
- 4. .
- 5. Definition A syndrome in which the respiratory system fails in one or both of its gas exchange functions i.e. oxygenation and/or carbon dioxide elimination, such that the levels of arterial oxygen (PaO₂) and carbon dioxide (PaCO₂) partial pressures cannot be maintained within their normal ranges. According to Lewis's
- 6. Respiratory failure is a condition in which your blood doesn't have enough oxygen or has too much carbon dioxide. Sometimes can have both problems. When you breathe, lungs take in oxygen. ... Your organs, such as heart ,lungs and brain, need this oxygen-rich blood to work well. According to Thomas Luckmann
- 7. Respiratory arrest should be distinguished from respiratory failure. The former refers to the complete cessation of breathing, while respiratory failure is the inability to provide adequate ventilation for the body's requirements According to Brunner & Suddarth's
- 8. Respiratory arrest and insufficiency: The condition in which the lungs cannot take in sufficient oxygen or expell sufficient carbon dioxide to meet the needs of the cells of the body. Also called pulmonary insufficiency. According to Lippincott Williams & Wilkins
- 9. The inability of the cardiac and pulmonary systems to maintain an adequate exchange of oxygen and CO2 in the Lungs. According to American nurses Dictionary
- 10. Components of the respiratory system Gas-exchange (Interface)organ • Lungs (parenchyma) • Blood vessels (pulmonary and bronchial) Ventilatory pump • Thoracic wall • Respiratory muscles • Brainstem and cortex • Anterior horn cells • Phrenic nerves and other nerves
- 11. TYPES
- 12. TYPES 1. Acute respiratory failure occurs when fluid builds up in the air sacs in lungs. When that happens, your lungs can't release oxygen into your blood. In turn, your organs can't get enough oxygen-rich blood to function. 2.Chronic respiratory failure is a condition that results in the inability to effectively exchange carbon dioxide and oxygen, and induces chronically low oxygen levels or chronically high carbon dioxide levels. Symptoms: Shortness of breath
- 14. 1.ACUTE RESPIRATORY FAILURE: Results from inadequate gas exchange for a short period. Insufficient O2 transferred to the blood Hypoxemia (type I) Hypoxemia refers to the low level of oxygen in blood, • Inadequate CO2 removal Hypercapnia (Type II Hypercapnia is a buildup of carbon dioxide in your bloodstream
- 15. Acute Respiratory Failure: CLASSIFICATION • HYPOXEMIC RESPIRATORY FAILURE(TYPE I) An arterial oxygen tension lower than 60 mm Hg with a normal or low arterial carbon dioxide tension. • HYPERCAPNIC RESPIRATORY FAILURE(TYPE II) CO2 higher than 50 mm Hg.
- 16. HYPOXEMIC RESPIRATORY FAILURE (TYPE I) CAUSES 1. Ventilation-perfusion (V/Q) mismatch 2. Shunt 3. Diffusion Limitation 4. Alveolar hypoventilation
- 17. 1. VENTILATION-PERFUSION (V/Q) MISMATCH: "V" – ventilation – the air that reaches the alveoli "Q" – perfusion – the blood that reaches the alveoli o COPD o Pneumonia o Asthma o Atelectasis o Pulmonary embolus
- 18. COPD: COPD stands for Chronic Obstructive Pulmonary Disease. It is a progressive disease that makes it hard to breathe. In COPD, less air flows in and out of the AIRWAYS BECAUSE OF ONE OR MORE OF THE FOLLOWING: •The airways and air sacs lose their elastic quality. •The walls between many of the air sacs are destroyed. •The walls of the airways become thick and inflamed. •The airways make more mucus than usual, which can clog them
- 19. PNEUMONIA: Pneumonia is an inflammatory condition of the lung. It is usually caused by infection with viruses or bacteria. ATELECTASIS: Partial collapse or incomplete inflation of the lung.
- 20. PULMONARY EMBOLISM is the sudden blockage of a major blood vessel (artery) in the lung, usually by a blood clot.
- 21. 2. SHUNT o Anatomic shunt o Intrapulmonary shunt
- 22. ANATOMIC SHUNT: Passes through an anatomic channel of the heart and does not pass through the lungs. INTRAPULMONARY SHUNT: Blood flows through pulmonary capillaries without participating in gas exchange.
- 23. 3. DIFFUSION LIMITATION: o Severe emphysema o Recurrent pulmonary emboli o Pulmonary fibrosis o Hypoxemia present during exercise
- 24. Severe Emphysema: Emphysema gradually damages the air sacs (alveoli) in your lungs, making you progressively more short of breath. Smoking is the leading cause of emphysema. Recurrent pulmonary emboli: Pulmonary embolism (PE) occurs when a blood clot dislodges from a vein, travels through the veins of the body, and lodges in the lung.
- 25. Pulmonary fibrosis: Pulmonary fibrosis occurs when lung tissue becomes damaged. This thickened, stiff tissue makes it more difficult for your lungs to work properly. Hypoxemia present during exercise: An abnormally low concentration of oxygen in the blood Recurrent Pulmonary embolism (PE) is a blockage of an artery in the lungs by a substance that has moved from elsewhere in the body through the bloodstream (embolism). Symptoms of a PE may include shortness of breath, chest pain particularly upon breathing in, and coughing up blood.
- 26. 4. ALVEOLAR HYPOVENTILATION: o Restrictive lung disease o CNS disease o Chest wall dysfunction o Neuromuscular disease
- 28. • HYPERCAPNIAC RESPIRATORY Failure (Type II) Causes : 1. Airways and alveoli. 2. Central Nervous System. 3. Chest Wall. 4. Neuromuscular Conditions
- 29. 1. AIRWAYS AND ALVEOLI: o Asthma. o Emphysema. o Bronchitis. o Cystic fibrosis.
- 30. . ASTHMA: A respiratory condition marked by attacks of spasm in the bronchi of the lungs, causing difficulty in breathing. It is usually connected to allergic reaction or other forms of hypersensitivity Emphysema: Emphysema gradually damages the air sacs (alveoli) in your lungs,
- 31. BRONCHITIS: Bronchitis is an inflammation of the bronchial tubes. CYSTIC FIBROSIS: A heriditary disorder causes the production of abnormally thick mucus, leading to the blockage of brunch.
- 32. 2. CENTRAL NERVOUS SYSTEM: o Drug overdose. o Brainstem infarction. o Spinal cord injuries 1. RESPIRATORY FAILURE is a common complication of drug abuse. ... Drugs may acutely precipitate respiratory failure by compromising respiratory pump function and/or by causing pulmonary pathology. Polysubstance overdoses are common, and clinicians should anticipate complications related to multiple drugs.
- 33. 2. BRAINSTEM INFARCTION (BSI) is a stroke that happens when blood cannot flow to your brainstem. When oxygen cannot get to an area of the brain, tissue in that area may be damaged. Your brainstem allows you to speak, hear, and swallow 3. SPINAL CORD INJURY (SCI) is damage to the spinal cord that causes temporary or permanent changes in its function. Symptoms may include loss of muscle function, sensation, or autonomic function in the parts of the body served by the spinal cord below the level of the injury.
- 34. 3. CHEST WALL: o Flail chest. o sternal fractures. o Muscle spasm 1. FLAIL CHEST is a life-threatening medical condition that occurs when a segment of the rib cage breaks due to trauma and becomes detached from the rest of the chest wall. Two of the symptoms of flail chest are chest pain and shortness of breath.
- 35. 2.STERNAL FRACTURE is a fracture of the sternum (the breastbone), located in the center of the chest. The injury, which occurs in 5–8% of people who experience significant blunt chest trauma, may occur in vehicle accidents, when the still- moving chest strikes a steering wheel or dashboard or is injured by a seatbelt.
- 36. 3. MUSCLE SPASM is a sudden, involuntary contraction of one or more muscles. A spasm results from an abnormally sustained muscle contraction and is often painful. Various muscles may develop spasms,
- 37. 4. NEUROMUSCULAR CONDITIONS: o Muscular Dystrophy. o Multiple Sclerosis. MUSCULAR DYSTROPHY is a group of diseases that cause progressive weakness and loss of muscle mass. In muscular dystrophy, abnormal genes (mutations) interfere with the production of proteins needed to form healthy muscle. .
- 38. MULTIPLE SCLEROSIS: Multiple sclerosis (MS) is a disease in which your immune system attacks the protective sheath (myelin) that covers your nerves. Myelin damage disrupts communication between your brain and the rest of your body. Ultimately, leading to respiratory failure and other diseases
- 40. CHRONIC RESPIRATORY FAILURE: The respiratory failure which passes the acute stage. All of the disorders are same, just the duration is lengthened.
- 41. CHRONIC RESPIRATORY FAILURE: Chronic respiratory failure is a condition that results in the inability to effectively exchange carbon dioxide and oxygen, and induces chronically low oxygen levels or chronically high carbon dioxide levels.
- 42. . •Tissue Organ Needs: Major threat is the inability of the lungs to meet the oxygen demands of the tissues. • Clinical Manifestations: A sudden decrease in O2 or rapid increase in CO2 indicates a serious condition
- 43. CLASSIFICATION HYPOXAEMIC (TYPE I) • Failure of oxygenation ↓ HYPOXEMIA without HYPERCAPNIA VENTILATORY (TYPE II) • Respiratory “PUMP” FAILURE ↓ HYPOXEMIA and HYPERCAPNIA
- 44. ETIOLOGY
- 45. 1. OBSTRUCTION When something lodges in your throat, you may have trouble getting enough oxygen into your lungs. Obstruction can also occur in people with chronic obstructive pulmonary disease (COPD) or asthma when an exacerbation causes the airways to become narrow. 2.INJURY An injury that impairs or compromises your respiratory system can adversely affect the amount of oxygen in your blood. For instance, an injury to the spinal cord or brain can immediately affect your breathing. The brain tells the lungs to breathe. If the brain can’t relay messages due to injury or damage, the lungs can’t continue to function properly. An injury to the ribs or chest can also hamper the breathing process. These injuries can impair your ability to inhale enough oxygen into your lungs.
- 46. 3. ACUTE RESPIRATORY DISTRESS SYNDROME Acute respiratory distress syndrome (ARDS) is a serious condition characterized by low oxygen in the blood. ARDS affects you if you already have an underlying health problem such as: pneumonia pancreatitis (inflammation of the pancreas) severe trauma Sepsis 4. SEVERE BRAIN INJURIES lung injuries caused by inhalation of smoke or chemical products It can occur while you’re in the hospital being treated for your underlying condition 5. DRUG OR ALCOHOL ABUSE If you overdose on drugs or drink too much alcohol, you can impair brain function and hinder your ability to breathe in or exhale.
- 47. 6.CHEMICAL INHALATION Inhaling toxic chemicals, smoke, or fumes can also cause acute respiratory failure. These chemicals may injure or damage the tissues of your lungs, including the air sacs and capillaries. 7.STROKE A stroke occurs when your brain experiences tissue death or damage on one or both sides of the brain. Often, it affects only one side. Although stroke does present some warning signs, such as slurred speech or confusion, it typically occurs quickly. If you have a stroke, you may lose your ability to breathe properly. 8. INFECTION Infections are a common cause of respiratory distress. Pneumonia in particular, may cause respiratory failure, even in the absence of ARDS. According to the Mayo Clinic, in some cases pneumonia affects all five lobes of the lungs.
- 48. PATHOPHYSIOLOGY
- 49. Hypoxaemic (Type I) • Pneumonia • ARDS • Pulmonary fibrosis • Asthma • COPD • Pnemothorax • PE • Obesity • Pulmonary Hypertension Hypercapnic (Type II) • COPD / Severe Asthma • Drug Overdose (Opiates benzodiazepines,) • CNS Injury (SCI, CVA) • Primary muscle disorders (Duchenne muscular dystrophy) • Neuromuscular junction disorders (eg. Myasthenia gravis) • Anatomical chest deformities (eg. Kyphoscoliosis, Flail chest) • Obesity Hypo-ventilatory (Pickwickian) syndrome DUE TO ETIOLOGICAL FACTORS SUCH AS
- 50. Failure of one and both gas exchange abnormal function oxygenation and co2
- 51. CLINICAL PRESENTATION RF may be preceded by signs of respiratory distress: • Tachypnoea (>25/min) • Breathlessness • Gasping or pursed lip breathingह ांफते हुए स ांस लेन • Tight chest • Sweating, • Agitation =a state of anxiety or nervous felling. • Sitting or hunched (swelling )posture • Sense of impending doom feeling fear • Inability to complete a sentences • Cyanosis • HYPOXAEMIA Sats • HYPERCAPNEA
- 52. PRE TERMINAL SIGN Signs of the pre-active dying phase include increased restlessness, being uncomfortable in one position, increased tiredness and periods of sleep, decreased food and liquid intake and oedema. • Bradycardia, • (dysrhythmias Cardiac dysrhythmias are a problem with the rate or rhythm of your heartbeat caused by changes in your heart's normal sequence of electrical impulses. heart may beat too quickly, called tachycardia; too slowly, bradycardia; or with an irregular heart pattern.), hypotension • Bradypnoea or silent chest • Decreased L.O.C ( level of consciousness )
- 53. PHYSICAL EXAMINATION 1) VITAL SIGNS AND INSPECTION • Fever, tachycardia, tachypnea → Infection • Fever, lethargy → CNS infection /septic encephalopathy • ↑Pulsus paradoxus (>10 mmHg) → Asthma or COPD
- 54. DIAGNOSTICS 2) NEUROLOGICAL EXAMINATION • Depressed mental status (lethargy or coma) → Central drive failure • Pupillary constriction (miosis) excessive constriction of the pupil of the eye. • “pinpoint pupils” → Opiate overdose (Severe hypercarbia causes miosis as well) • Sensory deficits → Polyneuropathy (e.g. GBS) • Muscle fasciculations → Motor neuron diseases (e.g. ALS)
- 55. DIAGNOSTICS 3) Head and Neck • Stridor, drooling → upper airway obstruction 4) Chest • Pattern of respiratory muscle contraction, chest diameter and intergrity (Flail chest), presence of abnormal breath sounds 5) Abdomen • Normal abdominal wall movement during inspiration is outward, inward movement with inspiration is paradoxical and suggests diaphragmatic fatigue.
- 56. DIAGNOSTICS Laboratory Testing 1. Arterial Blood Gas (ABG) An arterial blood gas (ABG) test measures oxygen and carbon dioxide levels in blood.
- 57. DIAGNOSTICS Normal values of arterial blood gases (at R.A., sea level, 37°C)
- 58. DIAGNOSTICS Interpretative remarks: • PaO₂ < 60mmHg(8kPa) →HYPOXEMIA • PaCO₂ > 50 mmHg(6.7 kPa) →HYPERCAPNIA • pH < 7.35 → ACIDOSIS • pH >7.45 → ALKALOSIS
- 59. DIAGNOSTICS 1. Complete Blood Count (CBC) • Leukocytosis → infection • Anemia (dyspnea,↓O₂ transport to tissues, but in isolation will not cause ventilatory failure. 2. Lumbar Puncture (LP) A lumbar puncture (spinal tap) is performed in lower back, in the lumbar region. During a lumbar puncture, a needle is inserted between two lumbar bones (vertebrae) to remove a sample of cerebrospinal fluid. This is the fluid that surrounds your brain and spinal cord to protect them from injury • (essential in cases of suspected CNS infection or GBS) 3. Serum Chemistries • (↓Ca,Mg,PO⁻ may contribute to respiratory muscle fatigue)
- 60. 4. TOXICOLOGY A toxicology screen is a test that determines the approximate amount and type of legal or illegal drugs that any person taken. It may be used to screen for drug abuse, to monitor a substance abuse problem, or to evaluate drug intoxication or overdose. Toxicology screening can be done fairly quickly.
- 61. 5.PULMONARY FUNCTION TESTS (PFTs) are noninvasive tests that show how well the lungs are working. The tests measure lung volume, capacity, rates of flow, and gas exchange. This information can help your healthcare provider diagnose and decide the treatment of certain lung disorders
- 62. DIAGNOSTICS Imaging and Other Tests • XRAY • (Pneumonia, atelectasis, pulmonary oedema, evidence of chronic lung disease, tumours, chest wall and pleural abnormalities) • CT Scan • (tumours, parenchymal lung disease, pleural and chest wall disease) • MRI • (encephalitis, brain stem pathology, and spinal cord injury) • ECG • (evidence of chronic lung disease, left ventricular failure or valve disease) • Last hai
- 63. MANAGEMENT Medical management Pharmacological management Surgical intervention Nursing management
- 64. MEDICAL MANAGEMENT Treatments for respiratory failure include the following: 1. Identification of causative agent 2. To give oxygen therapy 3. To maintain nutritional diet 4. Inhaled medications: Medicines administered either through an inhaler device or through a nebulizer machine can also open up airways, allowing lungs to pick up oxygen and remove carbon dioxide more effectively.
- 65. OXYGEN THERAPY: Face mask. Nasal canula.
- 66. 2. Drug Therapy: Use of Bronchodilators, Anti-biotics • DRUGS: • Respiratory stimulants (eg. Doxapram) Doxapram is an analeptic agent (a stimulant of the central nervous system). The respiratory stimulant action is manifested by an increase in tidal volume associated with a slight increase in respiratory rate.(rarely used) • Antidote for sedative overdose » Opioids → naloxone » Benzodiazepines → Flumazenil 3. Nutritional Therapy: •Maintain protein and energy stores
- 67. Principles of treatment • Emergency treatment should follow principles of cardiopulmonary resuscitation (C-A-B); • Ensure patent airway • Administer oxygen to maintain sats >90% • Correct hypoperfusion/anaemia followed by treatment of underlying (reversible) causes: • Acidosis/Alkalosis • Hypovolemia • Hypoxia • Pneumothorax • Pulmonary embolism
- 68. Principles of treatment (Cont…) • All patients with acute VF not responding to simple measures in an emergency room, clinic, or hospital ward setting should be monitored in an intensive/intermediate care unit. • Inhaled bronchodilators should be administered to all patients with bronchospasm. • Fever reduction with acetaminophen will decrease CO₂ production. • Avoid excessive caloric intake (which increases CO₂ production)
- 69. The main goal of treating respiratory failure is to get enough oxygen to your lungs and organs and remove carbon dioxide. Treatments for respiratory failure include the following: Inhaled medications: Medicines administered either through an inhaler device or through a nebulizer machine can also open up airways, allowing your lungs to pick up oxygen and remove carbon dioxide more effectively.
- 70. Con… The underlying cause may also require treatment - for example, steroids and antibiotics. For some patients there may not be any further treatment options and their respiratory failure may be terminal. They may benefit from the palliative care team, which deals with managing patients with terminal illnesses.
- 72. Principles of treatment (Cont…) • Consider non-invasive ventilatory support: • CPAP: continous positive airway pressure • BiPAP: Biphasic positive airway pressure • Evaluate patient for the need of Endotracheal intubation and mechanical ventilation (e.g. in cases of severe respiratory failure with PaO2 Partial pressure of oxygen (PaO2). less than 50 mmHg).
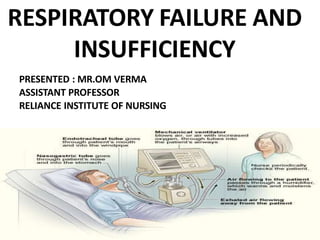
- 73. Tracheostomy: involves surgically creating a hole in the front of cleint neck and into windpipe. A tube called a tracheostomy is put into the hole to improve your breathing. You may also receive oxygen therapy through a tracheostomy Ventilator: is used when blood oxygen levels do not increase with oxygen therapy or tracheostomy alone. A ventilator is a machine that helps you breathe. It blows air into your airways and lungs. Non-invasive Positive Pressure Ventilation (NPPV): is a noninvasive treatment that helps to keep airways open while you sleep. NPPV involves wearing a mask that creates mild air pressure to keep the airways open. Fluids: Having the correct amount of fluid in the body supports proper blood flow and transportation of nutrition throughout the body, without causing fluid to build up in the lungs. You may be given fluids intravenously to ensure have just the right amount. This is usually done if are in the hospital.
- 74. Oxygen - high levels will be given through a mask (although lower levels may be needed in patients with chronic respiratory failure who have adapted to high carbon dioxide levels). Artificial ventilation: MECHANICAL VENTILATION: This involves the patient being put into a coma, using medication and paralyzing their breathing. A tube is inserted into the trachea and an artificial ventilator then does the work of breathing. Once the underlying cause is treated, patients will be 'weaned' off the ventilator so that their lungs start to do the work of breathing. This is a form of 'invasive' ventilation.
- 75. COMPLICATION
- 76. As a result of respiratory failure various complications can occur, including: Lung complications: for example, a blood clot on the lung (pulmonary embolism), irreversible scarring of the lungs (pulmonary fibrosis), a collection of air between the lung and chest wall (pneumothorax) which can further compromise breathing, chronic respiratory failure and dependence on a ventilaton
- 77. CON……. Heart complications: for example, heart failure, fluid around the heart (pericarditis) and acute heart attack
- 78. Increase in blood count (called polycythaemia): the increased level of red cells occurs from low blood oxygen levels but can lead to blood clots, due to sluggish flow in the blood vessels. Neurological complications: a prolonged period of low blood oxygen levels can deprive the brain of oxygen, which may be irreversible and may present as coma, fits (seizures) and even brain death.
- 79. Prolonged hospital admissions can lead to the following complications: Hospital-acquired infections: for example, pneumonia and diarrhoea. A pneumonia is likely to put further strain on the respiratory function and can require a need for further ventilation. Complications from being bed bound for long periods: wasting of limbs with associated weakness, pressure sores, deep vein thrombosis and mental depression
- 80. Prolonged hospital admissions can lead to the following complications: Hospital-acquired infections: for example, pneumonia and diarrhoea. A pneumonia is likely to put further strain on the respiratory function and can require a need for further ventilation. Malnutrition which may require assisted feeding methods, such as a tube being inserted down the nose into the stomach (nasogastric feeding), or providing nutrition through a needle straight into the bloodstream. Both of these methods have complications of their own. Complications from being bed bound for long periods: wasting of limbs with associated weakness, pressure sores, deep vein thrombosis and mental depression