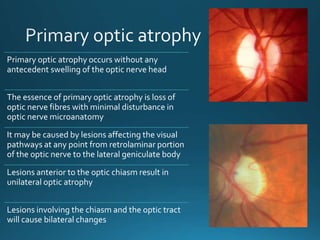
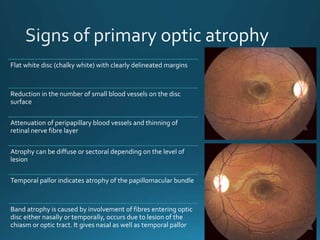
Primary optic atrophy occurs due to direct damage to the optic nerve and results in chalky white disc color with well defined margins and normal cupping and vessels. Secondary optic atrophy follows conditions like papilledema that cause swelling first, resulting in a filled cup and dirty white color. Consecutive optic atrophy occurs after other retinal conditions and shows waxy pallor, normal cup and grossly thinned vessels.