
Recommended
More Related Content
What's hot
What's hot (20)
Similar to MEDICATION-RELATED OSTEONECROSIS OF THE JAWS (MRONJ
Similar to MEDICATION-RELATED OSTEONECROSIS OF THE JAWS (MRONJ (20)
More from Hadi Munib
More from Hadi Munib (20)
Recently uploaded
Recently uploaded (20)
MEDICATION-RELATED OSTEONECROSIS OF THE JAWS (MRONJ
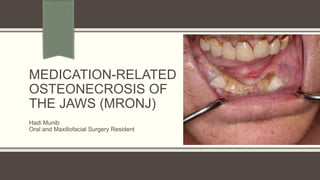
- 1. MEDICATION-RELATED OSTEONECROSIS OF THE JAWS (MRONJ) Hadi Munib Oral and Maxillofacial Surgery Resident
- 2. Outline Medication-Related Osteonecrosis of the Jaws Osteomyelitis of the Jaws References
- 3. AAOMFS Definition in 2022 Update Current or previous treatment with antiresorptive therapy alone or in combination with immune modulators or antiangiogenic medications. Exposed bone or bone that can be probed through an intraoral or extra-oral fistula(e) in the maxillofacial region that has persisted for more than eight weeks. No history of radiation therapy to the jaws or metastatic disease to the jaws. Anatomic Factors: Mandible 75% Maxilla 25% Both Jaws 4.5%
- 4. Predisposing Factors Dentoalveolar Surgery; the most common identifiable predisposing factor for developing MRONJ 62-82% Concomitant Oral Disease; a risk factor among 50 percent of the cases. Trauma Smoking Steroids, Immunocompromised host Autoimmune diseases Diabetes Chemotherapy.
- 7. Multiple Myeloma Patient on Zometa
- 9. Patient with Maxillary MRONJ
- 10. CT Scans
- 11. C-Terminal Telopeptide Test (CTX) Female (premenopausal): 40-465 pg/mL. Female (postmenopausal): 104-1008 pg/mL. Male: 60-700 pg/mL. Elevated levels are found in osteoporosis patients with elevated bone turnover who are at increased risk for rapid disease progression. Increased levels are also associated with osteopenia, Paget disease of the bone, hyperthyroidism, and hypothyroidism.
- 12. C-Terminal Telopeptide Test The risk of MRONJ following a dental procedure in patients on bisphosphonates was High if the CTX level was below 100 pg/ml Moderate at 100–150 pg/ml Low above 150 pg/ml
- 13. Is CTX a reliable Marker?
- 14. Is CTX a reliable Marker
- 15. Different Names ARONJ; Anti-Resorptive -induced osteonecrosis of the jaws. DIRONJ; drug-induced osteonecrosis of the jaws. MRONJ; medication-induced osteonecrosis of the jaws. Zoledronic acid, the most potent bisphosphonate.
- 16. Bisphosphonates Antiresorptive medications that are effective in managing cancer-related conditions Including hypercalcemia of malignancy, spinal cord compression and pathologic fractures associated with bone metastases in the context of solid tumors (such as breast, prostate and lung cancers) and multiple myeloma. Used for the prevention of osteoporosis-related fractures (fragility fractures) BPs administered: Orally including alendronate (Fosamax), risedronate (Actonel) Parenterally (zoledronic acid [Reclast]), and ibandronate (Boniva) Can result in a significant reduction in vertebral and non-vertebral fractures for patients with osteoporosis
- 17. Definition Bisphosphonates Work by: 1. Inhibition of osteoclast recruitment 2. Reduction of osteoclast life span 3. Inhibition of osteoclastic activity at the bone surface. Bisphosphonate medications can also be used to treat Paget’s disease of bone and osteogenesis imperfecta. Bisphosphonates inhibit osteoclast activity and prevent bone breakdown. Bisphosphonates also affect osteoblast activity, secondarily affects osteoclast activity. The half-life of this medication is long, measured in years.
- 18. Patients About to Initiate Bisphosphonate Therapy The goal in this group is to prevent the development of ONJ. If at all possible, the initiation of bisphosphonate therapy should be delayed until oral/dental health is optimized. Non-restorable teeth and teeth with poor prognoses should be extracted. It is recommended to allow 14–21 days to allow adequate healing before starting bisphosphonate therapy. [2 months American Guidelines] Restorative dentistry, scaling, and prophylaxis are best completed before initiation of bisphosphonate therapy. Patients should be educated about the importance of good oral and dental hygiene. Routine dental examinations and evaluations are important to monitor patient compliance and to detect problems early rather than at a later stage.
- 19. Patients Receiving Bisphosphonate Therapy Patients should maintain good oral and dental hygiene in order to prevent problems that require osseous surgery. Dental procedures that involve bony surgery should be avoided. Endodontic therapy is preferable to extraction of teeth. Placement of dental implants should be avoided. The incidence of developing ONJ in patients receiving intravenous bisphosphonates is higher than in patients receiving oral bisphosphonate therapy
- 20. Root Canal is Preferable to Extraction
- 21. Root Canal is Preferable to Extraction
- 22. Patients Receiving Oral Bisphosphonates The risk of ONJ appears to be associated with a longer duration of therapy, 3 years or greater. In patients who have taken oral bisphosphonates for less than 4 years and have no clinical risk factors, no alteration in the planned dento-alveolar treatment is required. Risk factors include conditions that may adversely affect healing, such as steroid treatment, diabetes and other medications, and medical conditions that would make the patient immunocompromised. In patients who have taken oral bisphosphonates for less than 4 years but have clinical risk factors, a “drug holiday” of at least 2 months should be considered before Dentoalveolar surgery.
- 23. Drug Holiday A pre-operative drug holiday of 3–6 months has been recommended for patients with a 3-year or greater history of bisphosphonate use
- 24. Collection of Position Papers for Controversy of Drug Holiday
- 25. Collection of Position Papers for Controversy of Drug Holiday
- 26. Collection of Position Papers for Controversy of Drug Holiday
- 27. In patients who have taken oral bisphosphonates for greater than 4 years (with or without risk factors), a drug holiday of 2 months should be considered before dentoalveolar surgery. Drug Holiday: Pre-Op: 2 months (American Guidelines) Pre-Op: 3-6 months (European and German) Post-op: 2 months (American Guidelines) Post-Op: 3-6 months (European and German) A total period of 6-9 months Patients Receiving Oral Bisphosphonates
- 29. Staging Patients at-Risk No apparent necrotic bone in asymptomatic patients who have been treated with IV or oral antiresorptive therapy.
- 30. Staging Stage 0 Patients with no clinical evidence of necrotic bone Nonspecific clinical and radiographic findings Pain and change in the bony trabecular pattern of the jaws; Dull, aching bone pain in the jaw, which may radiate to the temporomandibular joint region. Progression to Stage 1 disease has been reported in up to 50 percent of patients with Stage 0 disease. Treatment Strategy Clinical follow-up is recommended with conservative treatment. Clinicians should provide symptomatic treatment such as pain control and manage any treatable condition such as dental caries and periodontal disease
- 31. Staging Stage 1; Patients have exposed and necrotic bone. Asymptomatic No sign of infection. Treatment Strategy Oral anti-microbial rinses; chlorhexidine 0.12%, are indicated. Close monitoring of the oral condition and maintaining good oral hygiene are recommended. Surgical treatment is generally not recommended. Sharp bony edges that are irritating oral tissues may be smoothed down.
- 32. Staging Stage 2: Patients have exposed and necrotic bone Symptomatic with pain and infection. Treatment Strategy Oral antimicrobial rinses are recommended in conjunction with antibiotic therapy. Penicillin is still effective in the management of MRONJ with infection. Quinolones, metronidazole, clindamycin, doxycycline, and erythromycin have been used empirically in penicillin-allergic patients. Refractory cases may require intravenous antibiotic treatment along with maintenance of suppressive treatment to manage the disease.
- 33. Staging Stage 3 Patients have exposed and necrotic bone Symptomatic with pain and infection and one or more of the following: Exposed and necrotic bone extending beyond the alveolar bone. Pathologic fracture. Extraoral fistula. Oral-antral or oral-nasal communication. Osteolysis extending to the inferior border of the mandible or maxillary sinus floor.
- 34. Staging – Stage 3 Management Surgical debridement, including resection, is used in conjunction with antibiotic treatment. Resection is generally reserved for extensive, late presentation of disease and pathologic fractures Mobile segments of bony sequestrum should be removed regardless of the disease stage. Care should be taken not to expose the uninvolved bone for fear of extending the disease process. Stopping intravenous bisphosphonates appears to offer no short-term benefit. Long-term cessation of bisphosphonate therapy may be beneficial in patient healing
- 35. Long-Term Follow-up Long-term patients were noted to have spontaneous fractures in their long bones, specifically the femur. Long term is felt to be greater than 5 years but some fractures occurred after 2 years of oral bisphosphonate therapy. These fractures occurred with walking and low-energy injuries. This has caused clinicians to reevaluate their recommendations for stopping oral bisphosphonate medications for a period of time(drug holiday) and allow the bone to resume a more normal state of resorption and deposition. The final therapeutic regimen of oral bisphosphonate therapy has yet to be determined.
- 36. Implants were placed 15 years ago
- 37. Stage 4 lung cancer 2 years ago and was treated with IV Zometa. Asymptomatic exposed bone around implants.
- 38. Mobile Segment and Implant resected
- 40. Pathologic Fracture In The Area
- 41. Planned Resection and Recon Plate
- 42. Intra-op Picture of Bone Graft and Remaining Mandibular Structure
- 44. Post-Op OPG
- 45. `
- 47. Operative Therapies for Mandibular MRONJ
- 48. Operative Therapies for Maxillary MRONJ
- 49. OSTEOMYELITIS
- 51. Three-dimensional CT scan showing bony sequestrum from low-grade osteomyelitis in lesion
- 52. Definition Inflammation of the bone marrow with a tendency to progression. It involves the adjacent cortical plates and periosteal tissues. The incidence of osteomyelitis is higher in the mandible due to the dense, poorly vascularized cortical plates and blood supply primarily from the inferior alveolar neurovascular bundle, a single source. Osteomyelitis is less common in the maxilla due to the excellent blood supply from multiple feeder vessels and less bone density.
- 53. Local and Systemic Factors Diabetes Autoimmune states Malignancy, malnutrition, Acquired immunodeficiency syndrome (AIDS). Medications such as steroids and chemotherapeutic agents. Local conditions; Osteopetrosis, bone pathology, and repeated surgeries can alter the blood supply to the area.
- 54. Pathogenesis Osteomyelitis primarily occurs as a result of contiguous spread of odontogenic infections, Dentoalveolar surgery and maxillofacial trauma. Any Dentoalveolar surgical procedure can potentially cause an osteomyelitis. The initial insult results in a bacteria- induced inflammatory process. In the normal healthy host, this process is self-limiting and is a component of the healing process With inflammation there is hyperemia and increased blood flow to the affected area Pus is formed when there is an overwhelming abundance of bacteria and cellular debris that cannot be eliminated by the body’s natural defense mechanisms. When the pus and subsequent inflammatory response occur in the bone marrow, an elevated intramedullary pressure is created which further decreases the blood supply to the area.
- 55. Pathogenesis Pus can travel via Haversian and Volkmann’s canals to spread throughout the medullary and cortical bone. Once pus has perforated the cortical plates and collects under the periosteum, the periosteal blood supply is compromised. Intra-oral or Extra-oral Fistula
- 56. Microbiology The major pathogenic species are streptococci and anaerobic bacteria; Staphylococcal species. The anaerobes responsible are generally bacteroides or peptostreptococci species. Often the infections are mixed species, growing several oral pathogens on final culture. Penicillin and metronidazole as dual drug therapy or clindamycin or Unasyn (ampicillin/sulbactam) Viral osteomyelitis has been reported
- 57. Classification Currently, there is no universally accepted classification system for osteomyelitis. Suppurative or Non-Suppurative by Lew and Waldvogel. Hematogenous or secondary to a contiguous focus of infection. Acute or Chronic by Hudson; the most advantageous Osteomyelitis is classified into acute and chronic forms based on the presence of the disease for a 1-month duration.
- 59. Clinical Presentation Pain; Deep and Boring Swelling and erythema of overlying tissues; Acute Osteomyelitis Adenopathy Fever; Acute Osteomyelitis Paresthesia of the inferior alveolar nerve with mandibular osteomyelitis; inflammatory process Trismus Malaise Fistulas
- 60. Garre’s
- 61. Laboratory Investigations Complete Blood Count with Differential C-Reactive Protein; Not Specific Erythrocyte Sedimentation Rate; Not Specific Radiographic Examination: OPG; Moth-Eaten Appearance CT; Gold Standard, requires 30–50% demineralization of bone before changes can be seen MRI; Early Stage of Osteomyelitis by loss of marrow signal before sequestration Nuclear Imaging; T-99 is very sensitive to areas of High turnover The addition of Gallium 67 or indium 111 as contrast agents, one can differentiate areas of infection from trauma or postsurgical healing.
- 62. Three-Phase T-99 Imaging Study The technologist starts imaging and injects the patient. Images are obtained at 1 to 3 seconds per frame (when using digital images) for a video clip lasting 60 seconds which is referred to as "dynamic imaging." This dynamic imaging demonstrates and characterizes relative perfusion to a particular area and is called the "flow phase" or "angiographic phase." Following this step, a second image is obtained in the same field of view and is termed the "blood pool" phase. This characterizes blood pool accumulation in the soft tissues and bone (or lack thereof) as a result of flow and capillary dilatation. Two to 3 hours after initial injection, the third phase, termed "delayed," includes images of the same location as the earlier phases and will also include either the whole body or the lower half of the body.
- 63. Terms A sequestrum is a segment of necrotic bone that becomes separated or “sequestered” from the healthy intact bone. The reactive bone that forms around the necrotic sequestrum is referred to as the Involucrum The draining tract extending from the skin to the sequestrum is termed the cloaca.
- 64. Lower Right 8 Post-Extraction OPG
- 65. Coronal and Axial CT Scan Cuts of the same case
- 67. Treatment Both medical and surgical interventions. In rare cases of infantile osteomyelitis, intravenous antibiotic therapy alone may eradicate the disease. Correct Diagnosis and Medical Evaluation Empiric antibiotic treatment should be started based on Gram stain results of the exudate. Definitive culture and sensitivity reports generally take several days or longer to be obtained.
- 68. Surgical Options Classic treatment is sequestrectomy and saucerization. The aim is to debride the necrotic or poorly vascularized bony sequestrum in the infected area and improve blood flow. Sequestrectomy involves removing infected and avascular pieces of bone Saucerization involves the removal of the adjacent bony cortices and open packing to permit healing by secondary intention. Decortication involves removal of the dense, often chronically infected and poorly vascularized bony cortex. It is often necessary to remove teeth adjacent to an area of osteomyelitis.
- 69. Surgical Options Fixation device (external fixator or reconstruction type plate) and/or placing the patient in maxilla-mandibular fixation is frequently used to prevent pathologic fracture. Some authors proposed adjunctive treatment therapy that deliver high doses of antibiotic to the area using antibiotic impregnated beads or wound irrigation systems. This therapy works on high local levels of antibiotics; the overall systemic load is very low, thus reducing the possible side effect and complication rate. Hyperbaric oxygen (HBO) treatment has also been advocated for the treatment of refractory osteomyelitis. HBO works on increasing tissue oxygenation levels that would help fight off any anaerobic bacteria present in these wounds
- 70. Surgical Options Resection of the jaw bone has traditionally been reserved as a last-ditch effort, generally after smaller debridement procedures have been performed or previous therapy has been unsuccessful or to remove areas involved with pathologic fracture. This resection is generally performed via an extra-oral route, and reconstruction can be either immediate or delayed based on the surgeon’s preference. Rigid internal fixation has simplified the postoperative course by providing a means for immediate function of the jaws. The custom milled plates are very precise and require little or no additional bending. The custom milled plates are stronger than traditional plates and are less prone to fracture. Inferior alveolar nerve preservation and immediate reconstructive surgery with bone grafts have shortened the clinical course for our patients
- 71. Chronic Pain and Swelling related to Lower Left 6
- 72. Post-Extraction OPG of LL6
- 73. Cutting guides fabricated based on CT scan and 3D printed model allows extremely accurate surgery
- 74. Bone Resection and Sequestration Excision
- 75. Reconstruction Plate and Preservation of Inferior Alveolar Nerve
- 76. Autogenous Bone Graft Placement
- 77. Question 1: MRONJ is more common in: A) Maxilla B) Mandible C) Both Jaws D) Other Bones in the human body
- 78. Question 2 A female patient presented to your practice complaining of Pain due to a badly decayed wisdom tooth, after history taking the patient has osteoporosis and she takes oral bisphosphonates for less than 4 years and with no clinical risk factors, extraction is planned for this Patient, which of the following statements is true regarding the planned procedure: A) Extraction is contraindicated in this case due to high risk of MRONJ B) No alteration in the planned dento-alveolar treatment is required. C) Prescribe Antibiotics and Analgesics and Defer the patient D) All of the above can be considered
- 79. References
- 80. References
- 81. THANK YOU!
Editor's Notes
- NOTE: To change the image on this slide, select the picture and delete it. Then click the Pictures icon in the placeholder to insert your own image.