
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Complement system Immunoglobulin
Similar to Complement system Immunoglobulin (20)
More from GovtRoyapettahHospit
More from GovtRoyapettahHospit (20)
Recently uploaded
Recently uploaded (20)
Complement system Immunoglobulin
- 1. Complement system Immunoglobulin Dept of Urology Govt Royapettah Hospital and Kilpauk Medical College Chennai Slides before 1st Section Divider complement system IMMUNOGLOBULIN S 1
- 2. Moderators: Professors: • Prof. Dr. G. Sivasankar, M.S., M.Ch., • Prof. Dr. A. Senthilvel, M.S., M.Ch., Asst Professors: • Dr. J. Sivabalan, M.S., M.Ch., • Dr. R. Bhargavi, M.S., M.Ch., • Dr. S. Raju, M.S., M.Ch., • Dr. K. Muthurathinam, M.S., M.Ch., • Dr. D. Tamilselvan, M.S., M.Ch., • Dr. K. Senthilkumar, M.S., M.Ch. Dept of Urology, GRH and KMC, Chennai. 2
- 3. The complement system plays an essential role in host defense against infectious agents and in the inflammatory process. Nomenclature: a. the first component of complement is named C1 (etc.) other components are designated by capital letters and names: Factor B, Properidin b. when cleaved: fragments of complement components are designated by small letters (e.g. C3a and C3b) 4 Dept of Urology, GRH and KMC, Chennai.
- 4. C3 C3a C3b Factor B Ba + Bb Factor H Factor I 5 Dept of Urology, GRH and KMC, Chennai.
- 5. Complement System Activation Amplification Biologic Function Regulation 6 Dept of Urology, GRH and KMC, Chennai.
- 6. Complement Pathways 3 pathways for activation: 1. classical: most specific (antibody dependent activation, binds C1) 2. lectin binding: some specificity (mannose binding protein, binds C4) 3. alternative: most primitive (non- specific, auto-activation of C3) 7 Dept of Urology, GRH and KMC, Chennai.
- 7. Activators Classical pathway Alternate pathway 1.Ag-Ab complex 2.Aggregated Ig 3.DNA 4.CRP 5.Trypsin 1.Bacterial endotoxins 2.IgA, IgD 3.CobraVenom 4.Nephritic Factor 8 Dept of Urology, GRH and KMC, Chennai.
- 8. Cascade: Many of the components are enzymes that become activated when cleaved into two peptides One peptide binds to the immune complex and becomes a functional part of it The other peptide diffuses away and can become an inflammatory mediator (binds to a receptor) 9 Dept of Urology, GRH and KMC, Chennai.
- 9. 10 Dept of Urology, GRH and KMC, Chennai.
- 10. Lectin pathway: ➢ Lectin: protein that binds to carbohydrate ➢ MBL binds to mannose (on many bacterial cells) ➢ MBL is produced by liver in acute-phase inflammatory reactions ➢ Once MBL binds to target cell, a serine protease (MASP) binds to it ➢ Acts like C1 11 Dept of Urology, GRH and KMC, Chennai.
- 11. C3a C3a increases the inflammatory response by binding to mast cells and causing them to release histamine 12 Dept of Urology, GRH and KMC, Chennai.
- 12. Building the C3 convertase or C5 activation complex After enough C3b is cleaved, the surface of the bacteria begins to become saturated with it. C2b and C4b which make up the C3 activation complex has a slight affinity for C3b and C3b binds to them When C3b binds to C2b and C4b it forms a new complex referred to as the C5 activation complex 13 Dept of Urology, GRH and KMC, Chennai.
- 13. The C5 activation complex The C5 activation complex (C2b, C4b, C3b) activates C5 proteins by cleaving them into C5a and C5b Many C5b proteins are produced by the C5activation complex. These C5b begin to coat the surface of the bacteria. 14 Dept of Urology, GRH and KMC, Chennai.
- 14. The function of C5a C5a disperses away from the bacteria. ◦ Binds to mast cells and increases inflammation. ◦ Most powerful chemotactic factor known for leukocytes 15 Dept of Urology, GRH and KMC, Chennai.
- 15. Building the Membrane Attack complex C5b on the surface of bacteria binds to C6 The binding of C6 to C5b activates C6 so that it can bind to C7 C7 binds to C8 which in turn binds to many C9’s Together these proteins form a circular complex called the Membrane attack complex (MAC) 16 Dept of Urology, GRH and KMC, Chennai.
- 16. Membrane Attack complex The MAC causes Cytolysis. ◦ The circular membrane attack complex acts as a channel in which cytoplasm can rush out of and water rushes in. The cells inner integrity is compromised and it dies 17 Dept of Urology, GRH and KMC, Chennai.
- 17. Functions of the complement system 18 Dept of Urology, GRH and KMC, Chennai.
- 18. Amplification: many C3 molecules are hydrolyzed 19 Dept of Urology, GRH and KMC, Chennai.
- 19. Alternative pathway 20 Dept of Urology, GRH and KMC, Chennai.
- 20. C3b Many C3b molecules are produced by the C3 activation complex. The C3b bind to and coat the surface of the bacteria. C3b is an opsonin ◦ Opsonins are molecules that bind both to bacteria and phagocytes ◦ Opsonization increases phagocytosis by 1,000 fold. Opsonins 21 Dept of Urology, GRH and KMC, Chennai.
- 21. Regulation of complement system ➢ Because it is nonspecific, several regulatory mechanisms are involved (otherwise there would be a lot of “collateral damage”) ➢ Many components are very labile ➢ Many regulatory proteins block activity through binding to target 22 Dept of Urology, GRH and KMC, Chennai.
- 22. Regulatory proteins Complement components Complement inhibitors Complement inactivators •Opsonin- C3b •MAC C5-C9 •Anaphylotoxin s-C5a, C3a • C1 esterase inhibitor(C1s INH) • S Protein • Factor I, • Factor H • Anaphylotoxi n inativator • C4 Binding Protein 23 Dept of Urology, GRH and KMC, Chennai.
- 23. Regulatory proteins Proteins Functions C1INH dissociates C1r2-C1s2 tetramer from C1q and stops activation of the classical pathway. C4BP binds to C4b and blocks binding of C2b Decay-accelerating factor (DAF) bind to C4b to block C4b/C2b complex formation displaces Bb from C3b accelerates decay of C3/C5 convertase. Factor I cleaves cell membrane–associated C3b into iC3b, C3d, and C3dg Factor H displaces Bb from the alternate pathway C3 convertase (C3bBb) 24 Dept of Urology, GRH and KMC, Chennai.
- 24. • CD59 • Membrane cofactor protein:This is a cofactor for factor I– mediated cleavage of C3b and C4b. • CR1:This is the receptor for C3b/C4b and has an inhibitory profile similar to DAF. • Properdin:This stabilizes AP convertases. • Clusterin:This blocks fluid phase MAC. • S protein:This blocks fluid phase MAC. • Anaphylatoxin inactivator:This inactivates C3a, C4a, and C5a. Regulatory proteins 25 Dept of Urology, GRH and KMC, Chennai.
- 25. Deficiency disorders Deficiency Disease DAF Paroxysmal Nocturnal hemoglobinuria C1 esterase deficiency Hereditary Angionerotic edema C1C2C4 SLE and collagen vascular disease C5 to C8 Gram negative diplococci infections, toxoplasmosis properdin, factor B, factor D Neisserial infections Factor H Hemolytic uremic syndrome C3 deficiency membranoproliferative glomerulonephritis 26 Dept of Urology, GRH and KMC, Chennai.
- 26. Summary: ➢The complement system comprises a group of serum proteins which, when activated, plays an important role in antigen clearance. ➢Elaborate regulatory mechanisms are required to prevent damage to normal cells. 27 Dept of Urology, GRH and KMC, Chennai.
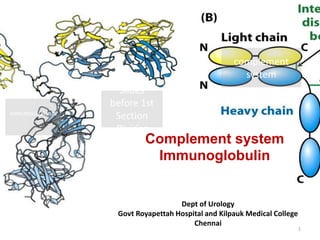
- 27. Antibody Structure Antibodies are globular proteins called Immunoglobulins (Ig) “Y”-shaped Made up of 4 polypeptide chains ◦ 2 identical heavy ◦ 2 identical light ◦ connected by disulfide bonds (-S-S-) 29 Dept of Urology, GRH and KMC, Chennai.
- 28. Antibody Structure Antibodies can also be divided into two regions based on their function ◦ Fab (fragment, antigen binding) region. Tip of the antibody Binds the antigen ◦ Fc (fragment, crystallizable) region Base of the antibody Can bind cell receptors, complement proteins and other molecules 30 Dept of Urology, GRH and KMC, Chennai.
- 29. Immunoglobulin domains • 4 (or 5) in heavy chain, • 2 in light chain. • Both heavy and light chains have one variable domain at the N- terminus chains held together by • disulfide bonds • noncovalent interactions 31 Dept of Urology, GRH and KMC, Chennai.
- 30. Variable regions are Site of antigen interaction Hypervariable (CDR; complementarity-determining region) site of antigen binding Rest of domain- framework 32 Dept of Urology, GRH and KMC, Chennai.
- 31. Constant-region domains CH1 and CL • stabilizeV regions • contribute to antibody diversity Hinge • flexibility • Fab and Fc can move around it • present in IgG, IgA, IgD • IgE and IgM have no hinge, instead • a fourth C domain 33 Dept of Urology, GRH and KMC, Chennai.
- 32. Antibody Isotype IgM – 1st class of circulating antibody - found in pentameric form IgG - most abundant antibody IgA - located in the mucous membranes - found in dimeric form IgD - found on surface of B-cells - probably involved in memory cell formation IgE - involved in allergies, i.e. trigger release of histamine 34 Dept of Urology, GRH and KMC, Chennai.
- 33. Ig isotypes differ in size, protein sequence and function 35 Dept of Urology, GRH and KMC, Chennai.
- 34. 36 Dept of Urology, GRH and KMC, Chennai.
- 35. IgG- most common in serum; monomeric four subclasses Slight differences in structure; significant differences in function 37 Dept of Urology, GRH and KMC, Chennai.
- 36. IgG1 and IgG3 are most active Fix complement Bind to Fc receptors on phagocytes opsonization IgG4 binds to Fc receptors; does not fix complement IgG2 fixes complement moderately; has low affinity for Fc rceptors IgG 38 Dept of Urology, GRH and KMC, Chennai.
- 37. IgM pentamer (or hexamer), so 10 antigen- binding sites produced in primary response 39 Dept of Urology, GRH and KMC, Chennai.
- 38. IgA • most common antibody in body- not serum, but in secretions. • Monomer in serum, multimer elsewhere • helps protect portals of entry in body • main protective antibody in breast milk 40 Dept of Urology, GRH and KMC, Chennai.
- 39. 41 Dept of Urology, GRH and KMC, Chennai.
- 40. IgE •Very low concentration in serum •Binds to Fc receptors on basophils and mast cells •induces hypersensitivity response 42 Dept of Urology, GRH and KMC, Chennai.
- 41. 43 Dept of Urology, GRH and KMC, Chennai.
- 42. IgD •Very low concentration in serum •Function of serum IgD is not known 44 Dept of Urology, GRH and KMC, Chennai.
- 43. Cytoplasmic part of membrane Ig is very short. 45 Dept of Urology, GRH and KMC, Chennai.
- 44. Humoral Immunodeficiency (B cells) 46 Dept of Urology, GRH and KMC, Chennai.
- 45. Primary B cell Deficiencies Genetic disorders of the B lymphocytes Approximately 70% of primary immunodeficiencies Not enough Ig or too much Ig X-Linked Agammaglobulinemia (XLA) Hyper IgM Syndrome Selective IgA deficiency ◦ Occurs in 1:600-1:800 people Development of anti-IgA antibodies may lead to severe anaphylactic reactions with blood transfusions 47 Dept of Urology, GRH and KMC, Chennai.
- 46. Humoral Immunodeficiency (B cells) Transient hypogammaglobulinemia of infancy ◦ Slow to develop normal levels of antibody ◦ Asymptomatic, minor infections ◦ Low levels of IgG, IgA (IgM usually normal) ◦ Resolves by 3-6 years IgA deficiency ◦ Most common humoral antibody deficiency ◦ 50-80% asymptomatic ◦ Recurrent sinopulmonary infections most frequent manifestation ◦ May have severe malabsorption (chronic diarrhea) ◦ Isolated low IgA level ◦ Increased risk of autoimmune disorders 48 Dept of Urology, GRH and KMC, Chennai.
- 47. Bruton’s X-linked Agammaglobulinemia No B cells Child clinically well for first 6 months of life Recurrent upper/lower respiratory tract infections with encapsulated bacteria (S. pneumo, H.flu) ◦ Bronchiectasis → chronic cough/increased sputum Sepsis, meningitis, skin infections Paucity of lymphoid tissue (tonsils, adenoids) Markedly decreased IgG, IgA, IgM Treatment: IVIG, antibiotic therapy 49 Dept of Urology, GRH and KMC, Chennai.
- 48. CommonVariable Immunodeficiency B lymphs don’t differentiate into plasma cells Recurrent sinopulmonary infections Low IgG, IgA, IgM Treatment: IVIG Associated with autoimmune disease, lymphoma 50 Dept of Urology, GRH and KMC, Chennai.
- 49. Combined Immunodeficiency 51 Dept of Urology, GRH and KMC, Chennai.
- 50. SCID Defects in stem cell maturation Adenosine deaminase deficiency (toxic insult to T and B cells) Manifestations seen in first 3 months of life ◦ Recurrent, severe bacterial, viral, fungal, and protozoan infections (usually respiratory infections) ◦ Failure to thrive, diarrhea, dermatitis, candidiasis Most have lymphopenia, decreased IgG, IgA, and IgM ◦ Diagnosis made by analysis ofT, B, and NK cell subsets Treatment: isolation, treat underlying infections, bone marrow transplant 52 Dept of Urology, GRH and KMC, Chennai.
- 51. Wiskott-Aldrich Syndrome X-linked recessive Symptoms in infancy ◦ Recurrent, severe infections ◦ Eczema ◦ Thrombocytopenia (petechiae) Low levels of IgM Increased risk for hematologic malignancy Treatment: manage bleeding/infections, BMT 53 Dept of Urology, GRH and KMC, Chennai.
- 52. Ataxia Telangiectasia Autosomal recessive deficiency in DNA repair affectingT and B cells Progressive ataxia, telangiectasia, variable immunodeficiency (recurrent sinopulmonary infections common) Increased risk of malignancy (leukemia, lymphoma) 54 Dept of Urology, GRH and KMC, Chennai.
- 53. Hyper IgE (Job) syndrome Autosomal recessive Symptoms/signs ◦ Coarse facial features/skeletal abnormalities ◦ Recurrent staph infections Impetigo (resistant) Pneumonia with pneumatocele formation ◦ 3 E’s: Elevated IgE, Eosinophilia, Eczema 55 Dept of Urology, GRH and KMC, Chennai.
- 54. Hyper IgM Syndrome T cell abnormality preventing IgM → IgG X-linked recessive (males 6 mo-1 year) Frequent sinopulmonary infections, diarrhea, opportunistic infections (PCP) Low levels of IgG/IgA, high levels of IgM Treatment: Ig replacement 56 Dept of Urology, GRH and KMC, Chennai.
- 55. 57 Dept of Urology, GRH and KMC, Chennai.
- 56. Summary of antibody features Basic structure: two identical heavy chains, two identical light chains Antigen-binding and effector functions Membrane-bound and secreted forms 58 Dept of Urology, GRH and KMC, Chennai.
- 57. 59 Dept of Urology, GRH and KMC, Chennai.