1) The document defines and describes the arterial pulse, its determinants, sites where it can be palpated, and characteristics including rate, rhythm, volume, and waveform.
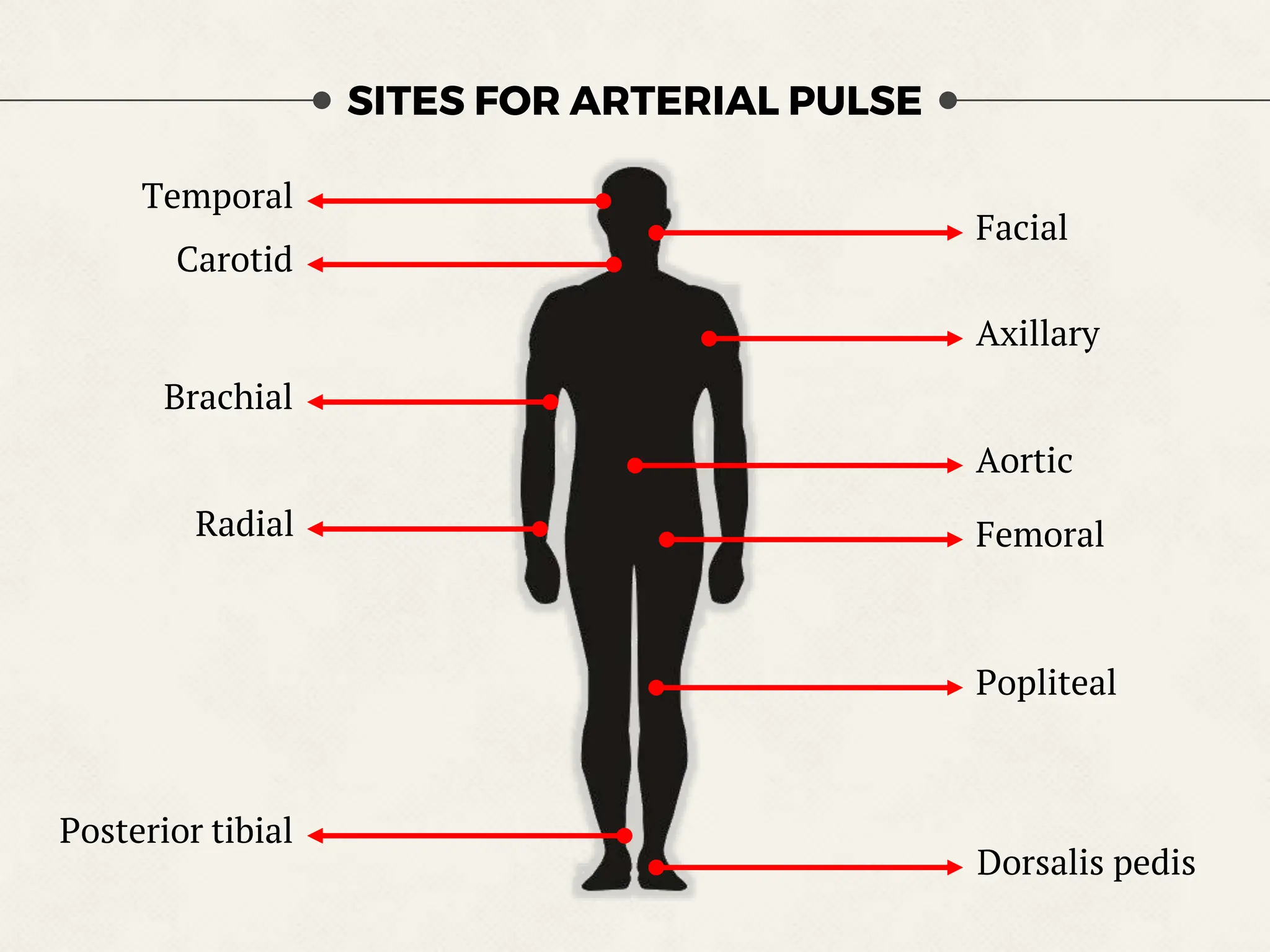
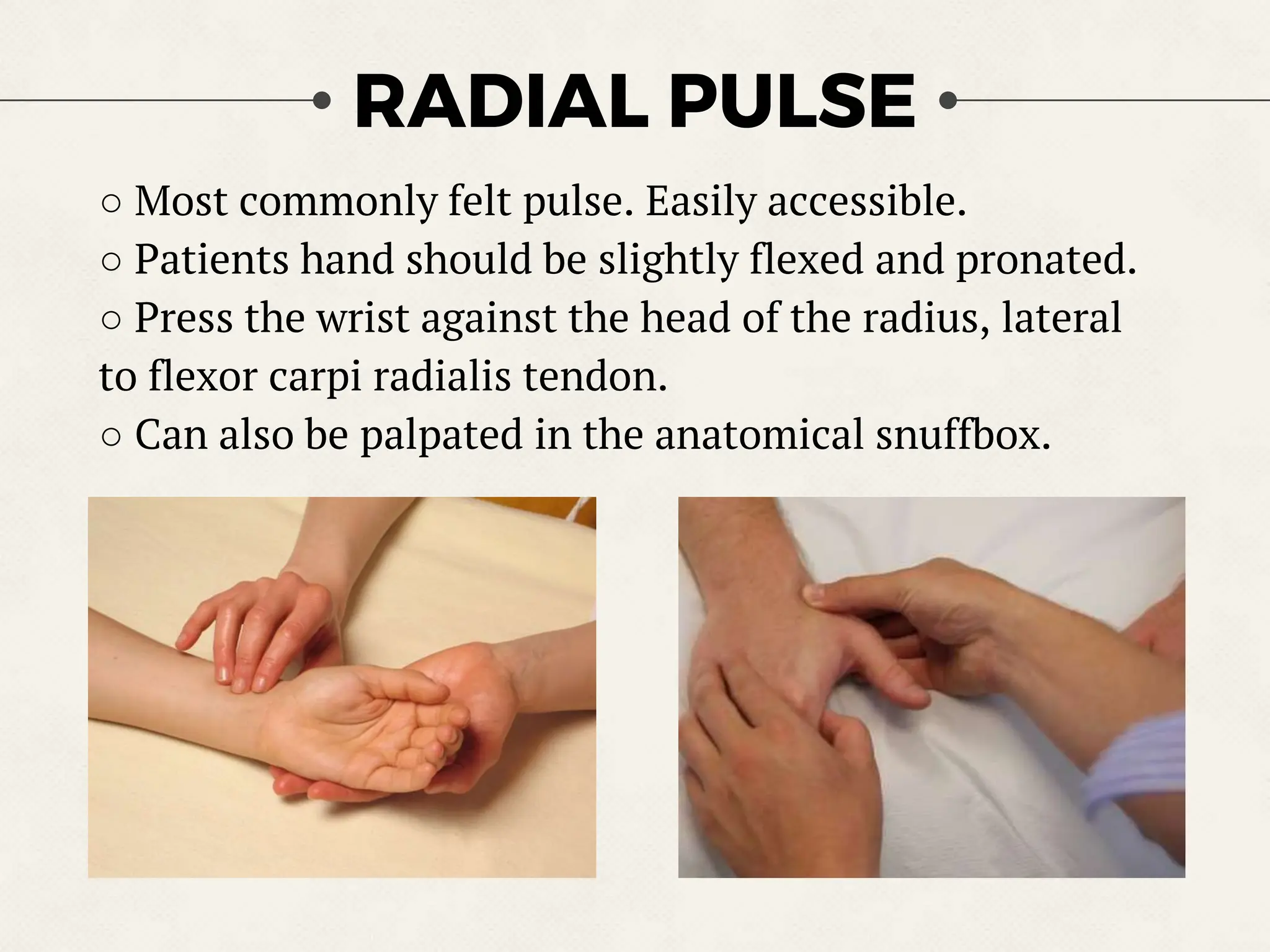
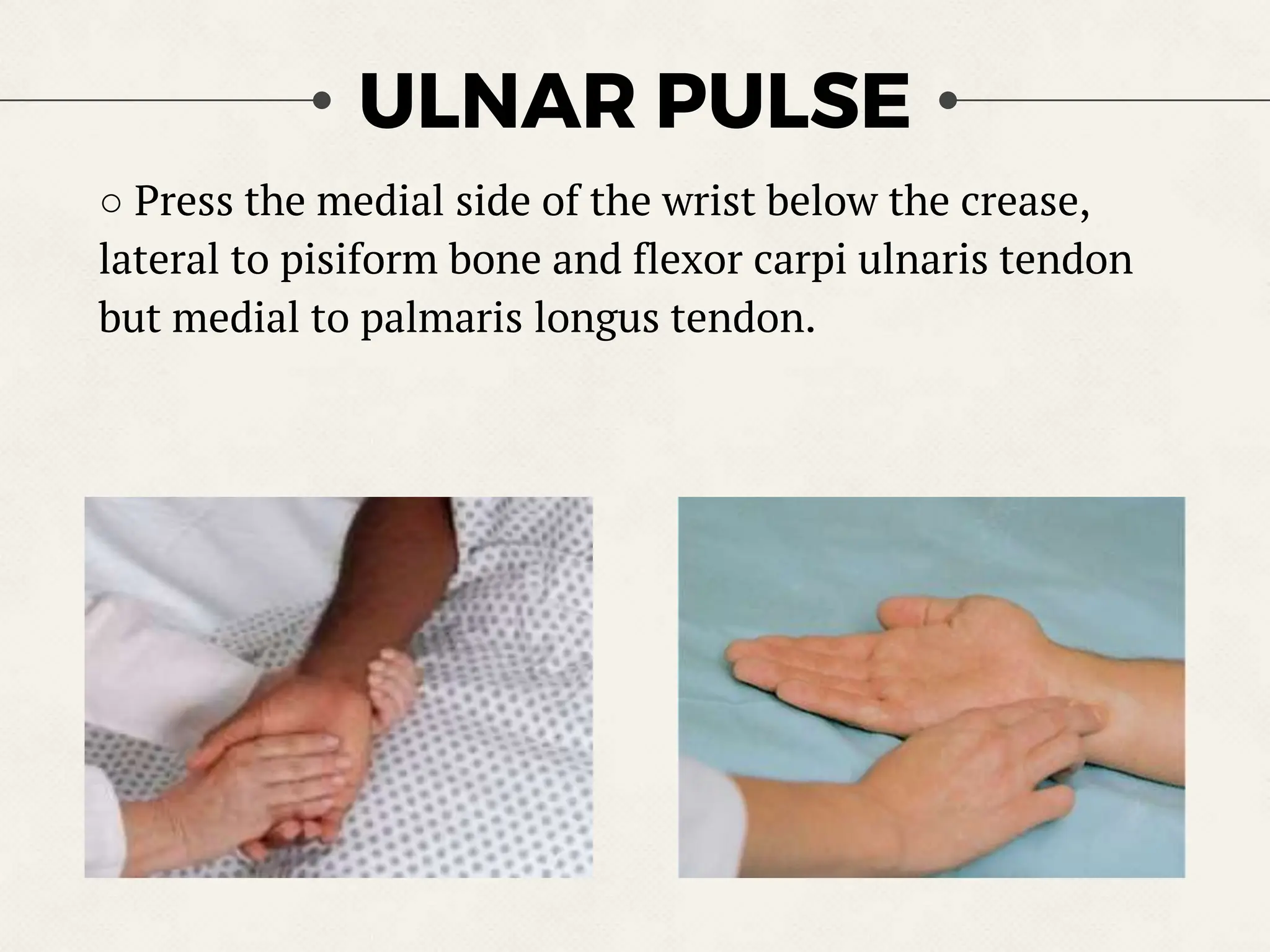
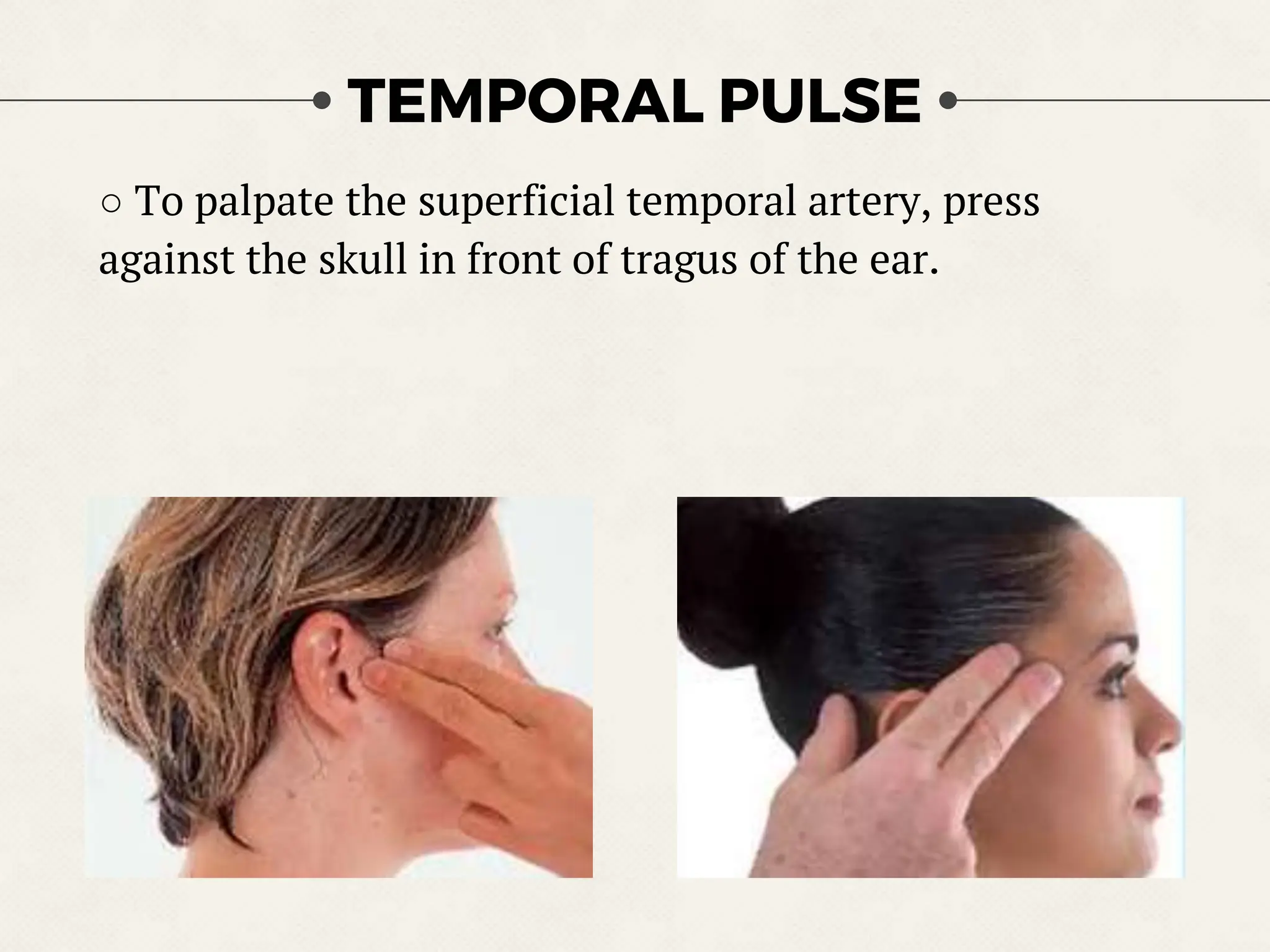
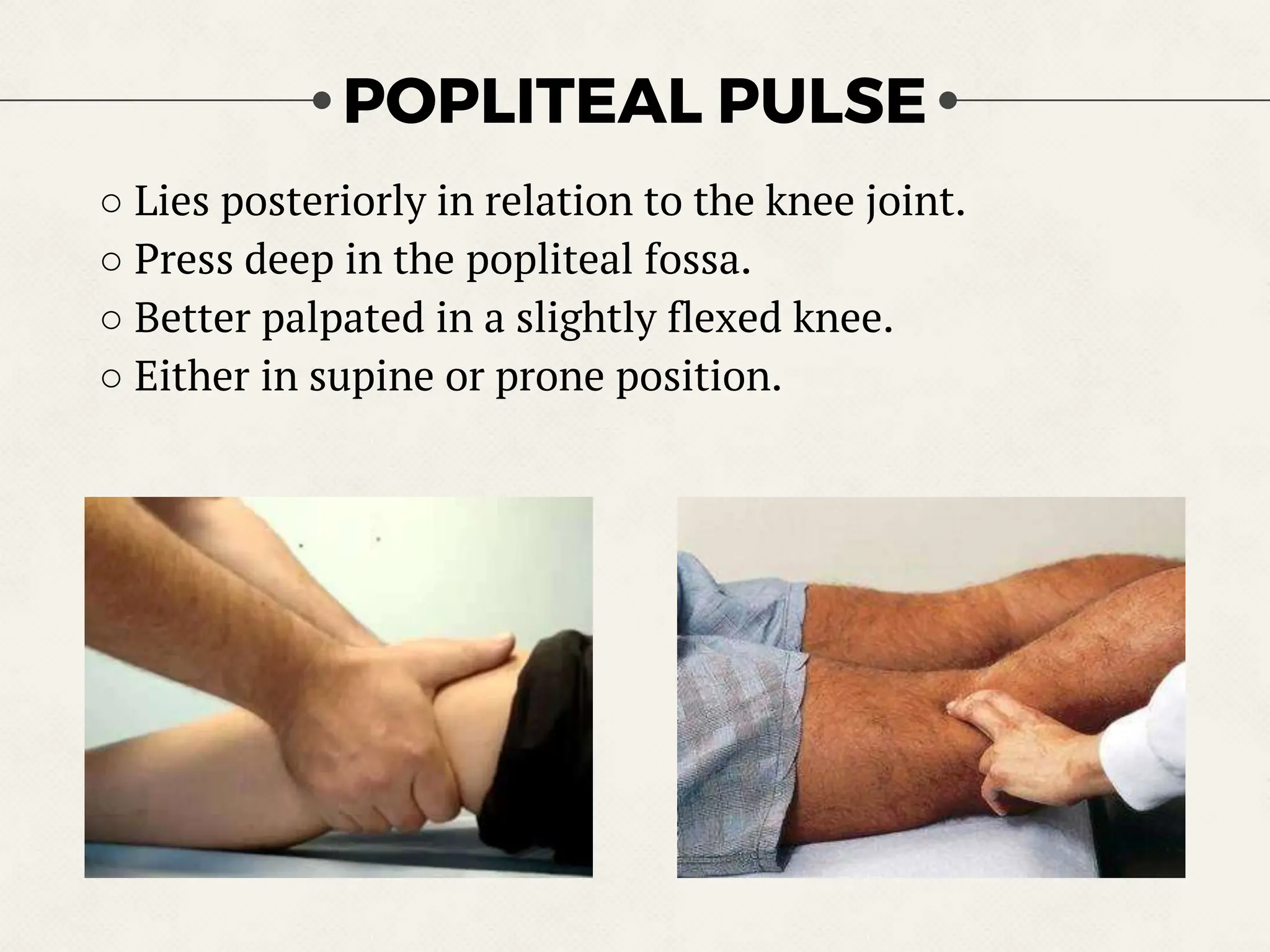
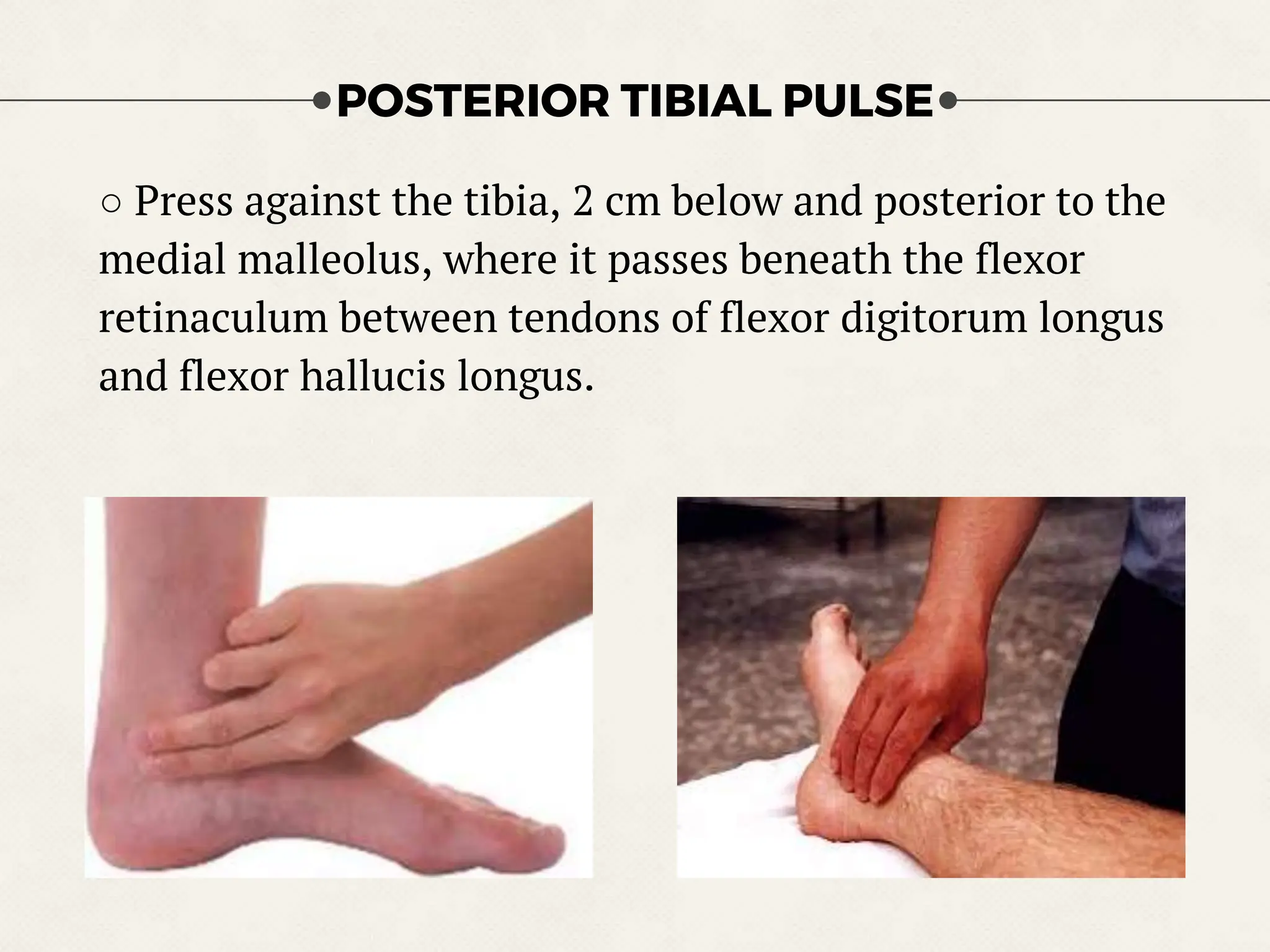
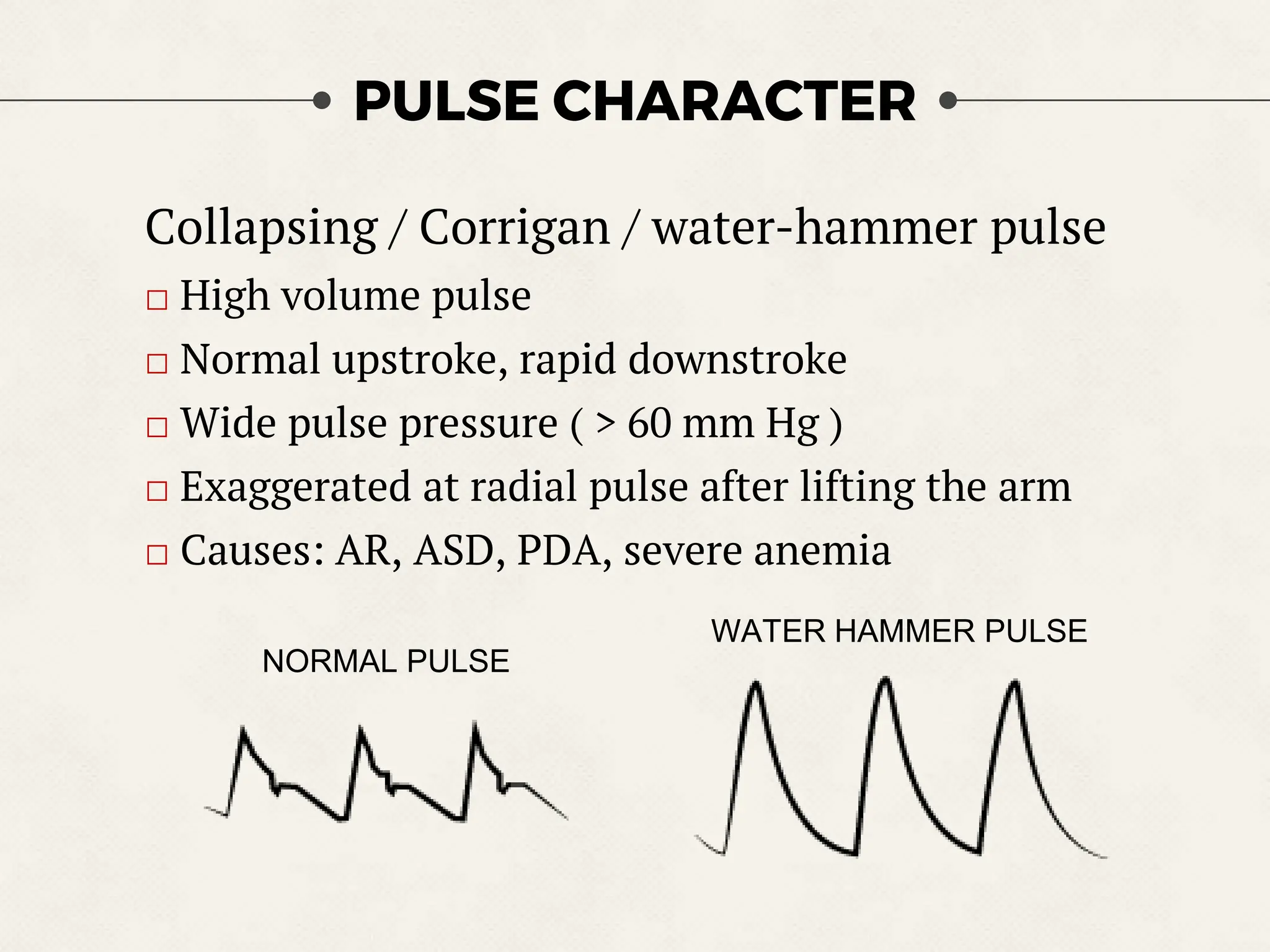
2) Key pulse points are described in detail including radial, brachial, carotid, femoral, and more. Characteristics of normal and abnormal pulse types are also outlined.
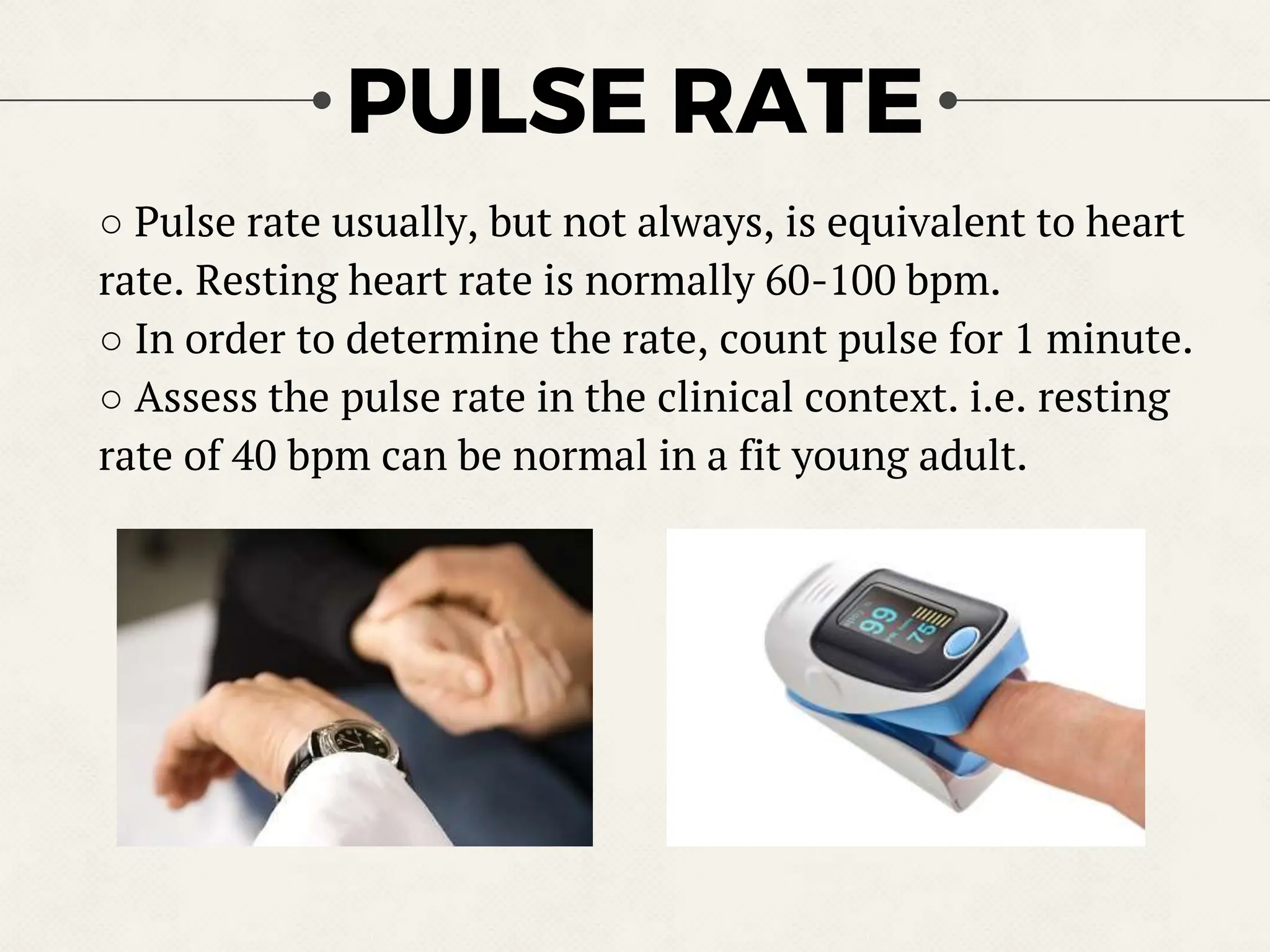
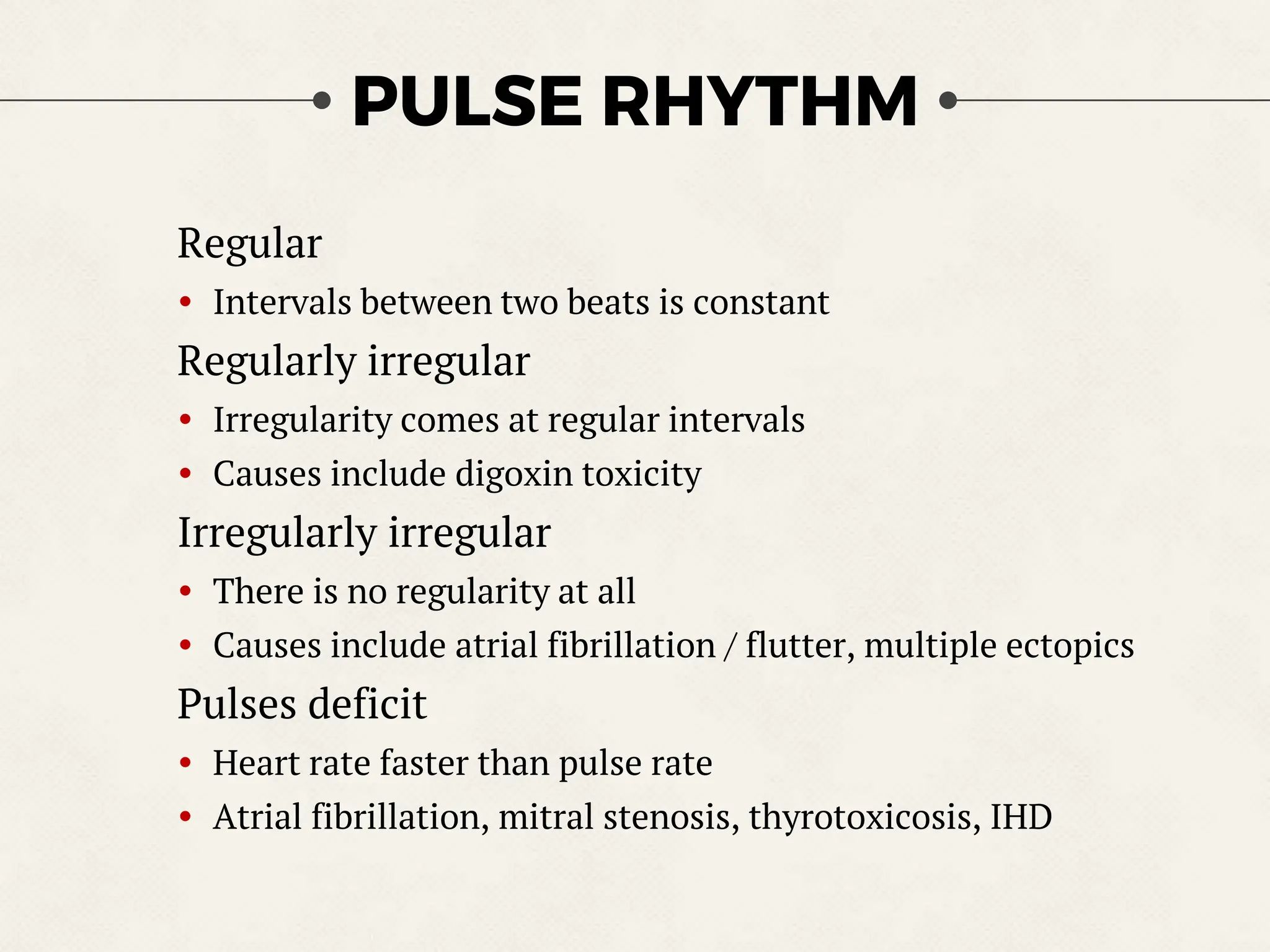
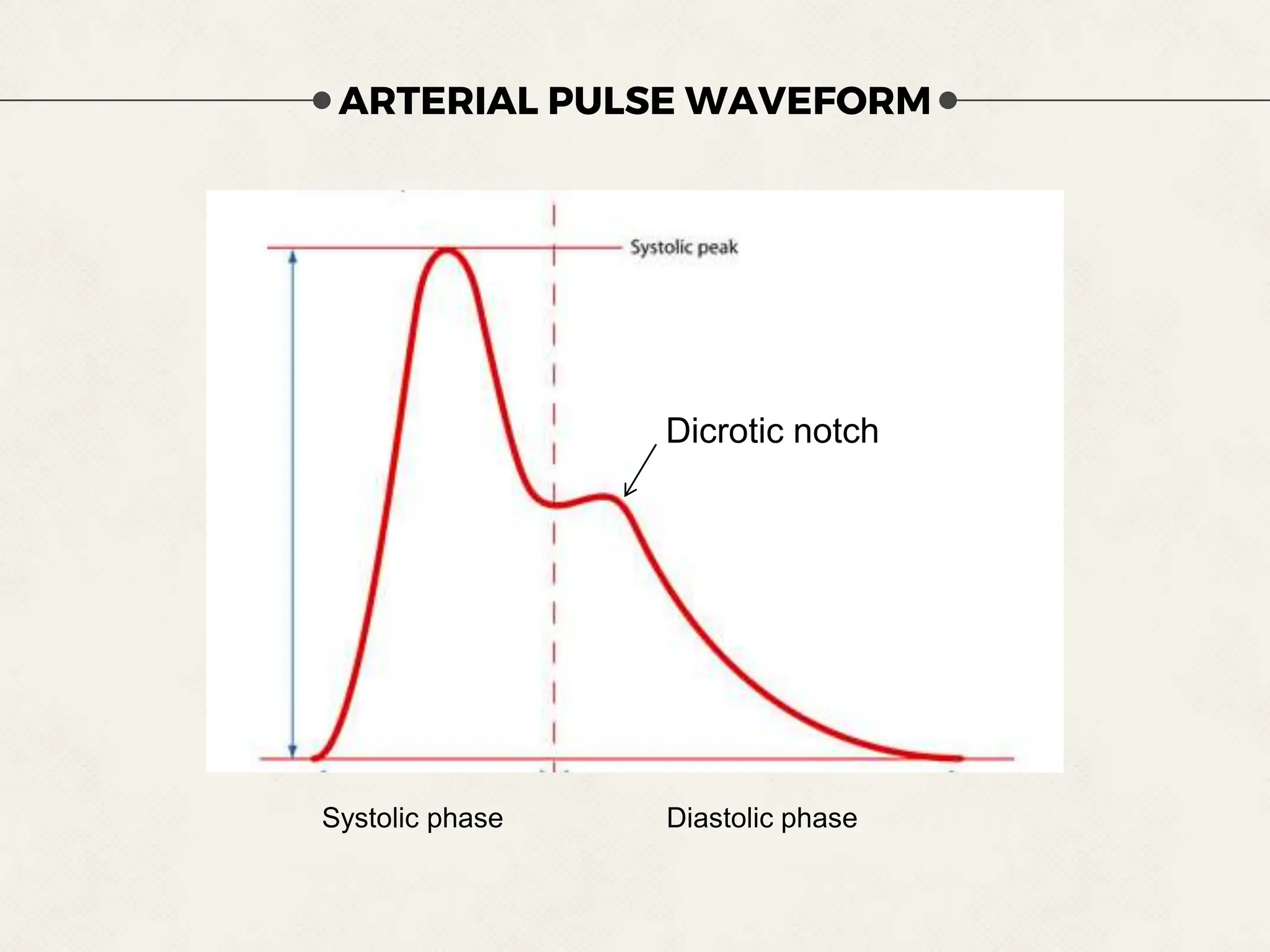
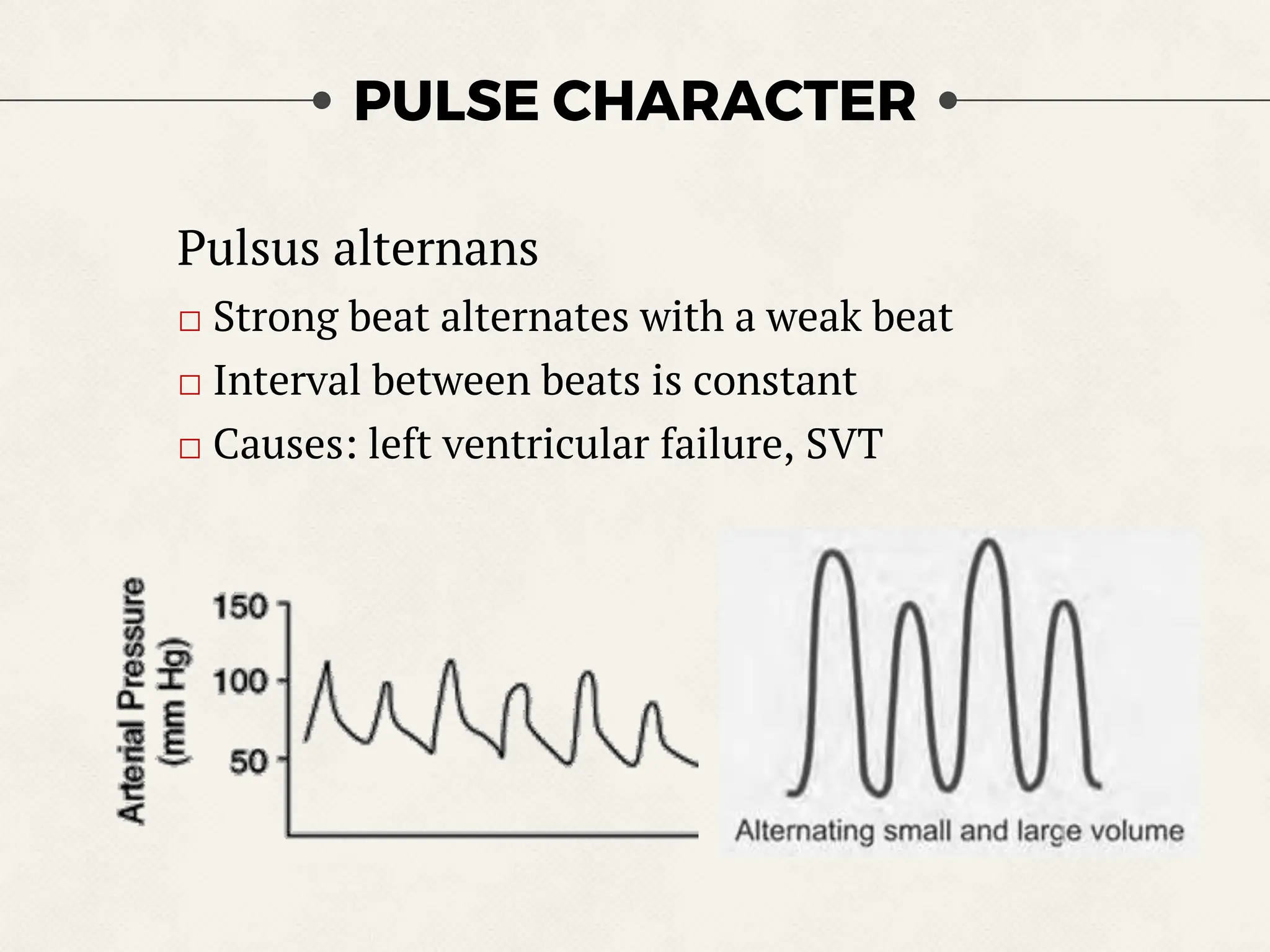
3) Assessment of pulse involves evaluating rate, rhythm, volume, and character, and comparing pulses at different sites can provide clinical information. Abnormal pulses may indicate various cardiovascular conditions.