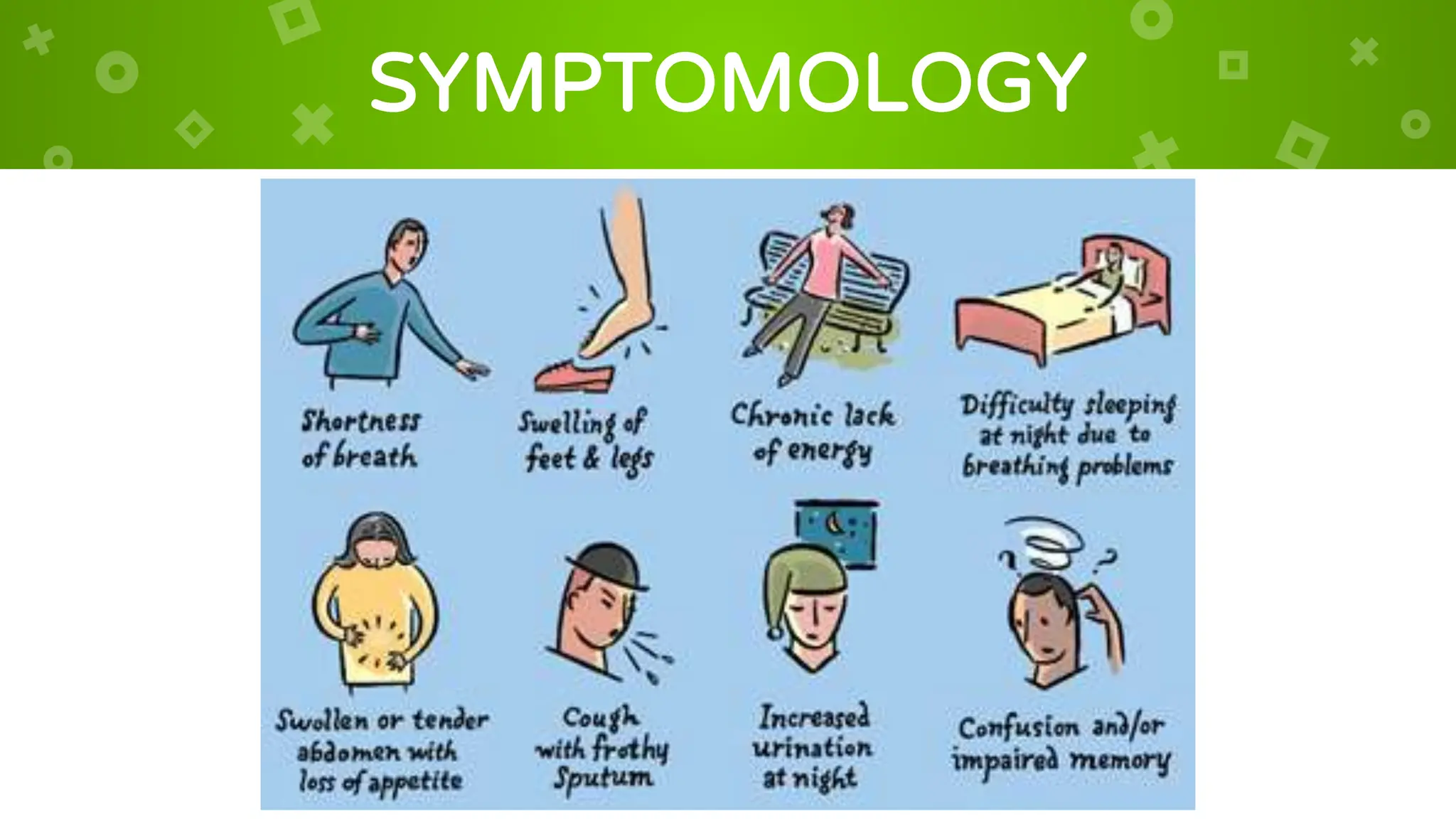
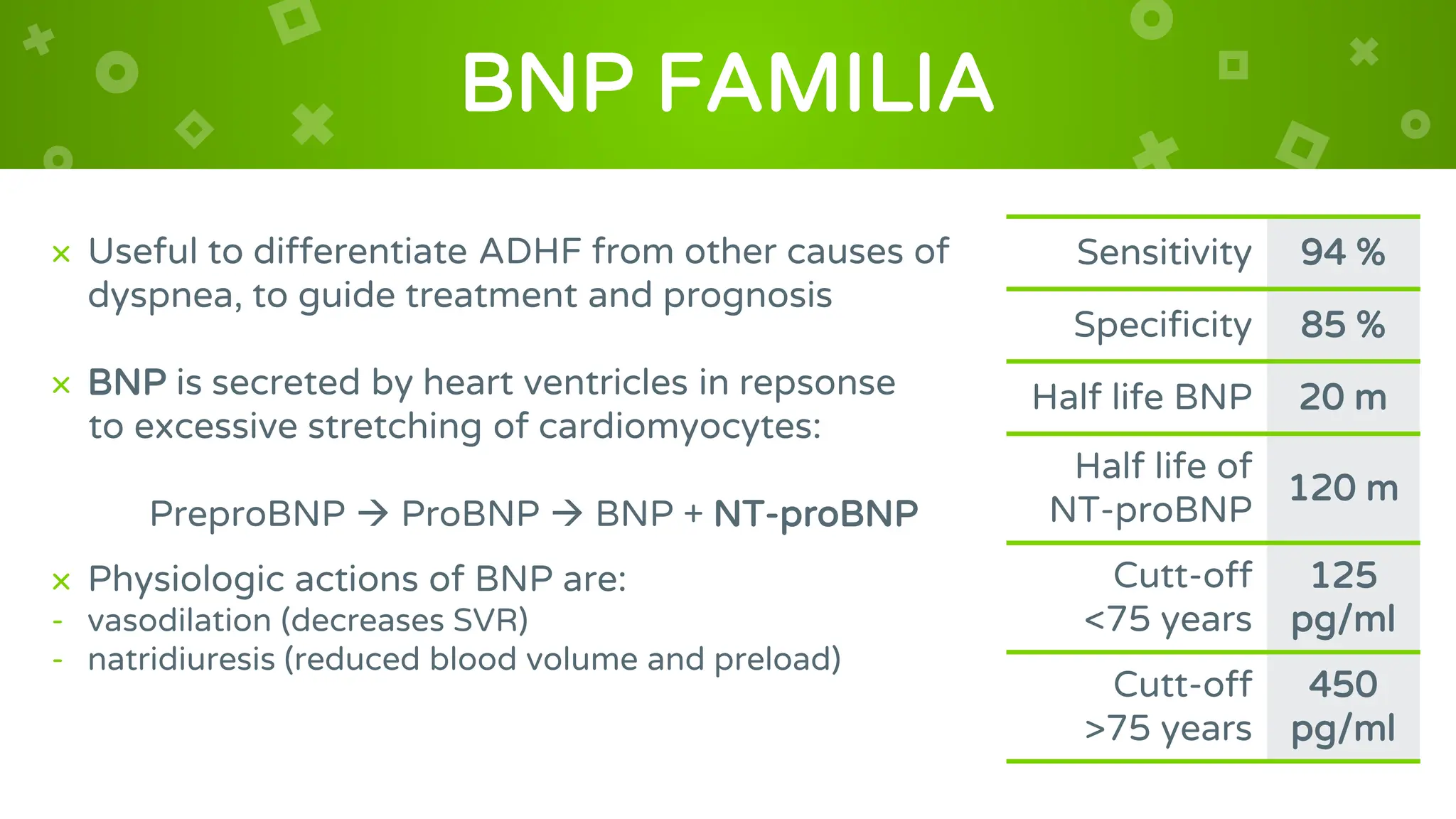
Heart failure occurs when the heart is unable to pump enough blood to meet the body's needs. It can be acute or chronic. Acute decompensated heart failure is a life-threatening condition characterized by increased filling pressures, pulmonary edema, reduced cardiac output, and organ dysfunction. Heart failure is determined by factors like contractility, heart rate, preload, and afterload. Preload refers to the stretch of heart muscle fibers before contraction and depends on factors like ventricular relaxation and compliance. Diastolic dysfunction can increase preload but also cause pulmonary congestion. Elevated natriuretic peptide levels help diagnose heart failure.