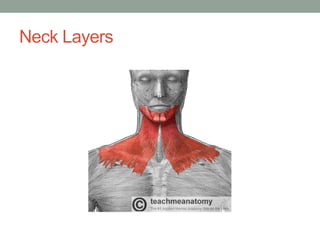
This document provides an overview of head and neck anatomy and clinical conditions. It discusses the neck triangles, lymph node distribution, blood supply, and neurology. It also covers how to examine the thyroid and parotid glands. Specific topics include the sinuses, facial nerve, skull anatomy, neck layers, and emergency airway management. Clinical pearls are provided about spread of infections, sinusitis, and evaluating lumps in the neck. Diagrams illustrate key anatomical structures like the neck triangles, carotid sheath, and lymph nodes.






![What’s in the Anterior triangle?
• Strap muscles: 3 further Triangles
• Common carotid artery bifurcates within the triangle
into the external and internal carotid arteries.
• The internal jugular vein also can be found within this
area. It drains blood from the head and neck.
• Facial [VII], Glossopharyngeal [IX], vagus [X],
• Accessory [XI], and Hypoglossal [XII] nerves.
• Lymph nodes
• Facial artery and vein (Submandibular traingle)
• Thyroid and Parathyroids](https://image.slidesharecdn.com/headandneckanatomy-131203133754-phpapp02/85/Head-and-neck-anatomy-11-320.jpg)