Top^Clinic ^%[+27785538335__Safe*Abortion Pills For Sale In Soweto
Buprenorphine Guidelines for Opioid Withdrawal in the Inpatient Psychiatry Unit.pptx
1. Bradford Unroe, MD, Gregory Ziomek, MD, Candace Jones, MD, Jessica Luo, DO, David Cho, MD, Blair Walker, MD, Sussann Kotara, MD
The University of Texas at Austin Dell Medical School, Department of Psychiatry and Behavioral Sciences
Introduction
● Opioid use disorder (OUD) has become a prevalent issue in
the United States, thus, it is imperative that physicians are
adequately trained for and confident in the treatment and
management of OUD and opioid withdrawal.
● At Seton Shoal Creek Hospital (SSCH), patients being
admitted with an active OUD diagnosis who are at risk for
opioid withdrawal or are currently in withdrawal are often
exposed to highly variable treatment approaches at the
beginning of their hospitalization. While buprenorphine, one of
the most effective and evidence-based treatments for OUD
and opioid withdrawal, is available at SSCH, guidance is
lacking on how to appropriately initiate buprenorphine during
the admissions process. Because of this and other suspected
buprenorphine prescribing barriers, it is also suspected that
prescriber confidence is low.
● Our goals were:
○ Create Buprenorphine for Opioid Withdrawal Admission
Order Guidelines
○ Identify barriers to prescribing buprenorphine
○ Assess prescriber confidence in prescribing
buprenorphine in the inpatient and outpatient setting
○ If prescriber confidence is low for the inpatient setting,
increase confidence with initiation and implementation of
opioid withdrawal guidelines
○ Assess satisfaction with the Buprenorphine for Opioid
Withdrawal Admission Order Guidelines
Methods
● Buprenorphine for Opioid Withdrawal Admission Order
Guidelines were created utilizing existing order sets used at
DSMC, recommendations from the literature, and expert
clinical opinion from Dr. Blair Walker and Dr. Sussann Kotara.
● All general psychiatry residents and attendings at UT Dell
Medical School Dept. of Psychiatry and Behavioral Sciences
were emailed a survey on 1/25/22 to be completed prior to
implementation of the guidelines on 2/15/22. This survey
asked questions such as history of and perceived barriers to
prescribing buprenorphine, satisfaction with current admission
order set for opioid withdrawal, and comfort in ordering
buprenorphine in the inpatient setting.
● They were then asked to complete the survey on 4/4/22
following implementation of the guidelines.
● Post-guideline implementation
○ 15 responses
○ Level of comfort in ordering buprenorphine in inpatient
setting; 93.3% responded 3-4/5, an increased of 86.6%:
○ Satisfaction with current opioid withdrawal admission
guidelines; 80% responded 3-4/5, an increase of 332%:
Discussion and Next Steps
By creating new opioid withdrawal guidelines we hoped to increase
prescriber comfort and satisfaction with a new SSCH admissions
order set, and we believed we partially accomplished that.
Challenges included data collection, as there were only 15
respondents for the post-implementation survey, and thus difficulties
in result interpretation. Given the improvement in confidence and
satisfaction observed, next steps include transitioning the opioid
withdrawal guidelines into a formal order within the SSCH
admissions order set. We intend to expand the feedback
assessment to other stakeholders involved in ordering
buprenorphine during the admissions process, such as Child and
Adolescent Psychiatry fellows and attendings and APPs, and over a
greater period of time. Subsequent goals can involve working with
SSCH utilization to assess actual provider ordering data and patient
adherence to buprenorphine for the treatment of OUD by analysing
the percentage of patients who are admitted with buprenorphine
ordered versus the percentage of patients who are discharged with
a buprenorphine prescription that is later filled.
Results
● Pre-guideline implementation survey
○ 28 responses
■ 88.9% reported prescribing buprenorphine in an
inpatient setting compared to 21.4% prescribing
buprenorphine in outpatient setting
■ 25% reported waivered by DEA to prescribe
buprenorphine
■ 92.6% were willing to apply for X-waiver
○ Barriers identified in ordering buprenorphine:
■ Lack of confidence in managing OUD (50%)
■ Low patient demand (28.6%)
■ Time constraints (25%)
○ Level of comfort ordering buprenorphine in inpatient
setting:
○ Satisfaction with current opioid withdrawal admission
order set:
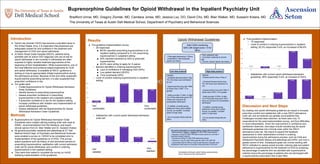
Opioid Withdrawal Guidelines
Buprenorphine Guidelines for Opioid Withdrawal in the Inpatient Psychiatry Unit
Not
comfortable
Very
comfortable
Not
satisfied
Very
satisfied
Start CINA monitoring
Q4hr with target score < 5 for
48hrs
- Prolonged abstinence (>72hrs)
- Intermittent, mild-moderate
opioid use history
- Prior suboxone use
- Comorbid moderate to severe
pain
- Chronic, severe opioid use history
Low dose protocol High dose protocol
ORDER:
- Schedule Buprenorphine 2mg
TID, first dose upon admission
to unit
- Buprenorphine 2mg q2hr PRN
(3 doses max) CINA = 5 or
greater
- Notify provider if CINA >5 after
1hr of 4mg total dose given OR
if there are concerns for
precipitated withdrawal*
- If notified, consider giving
additional 4-8mg with multiple
rounds, as needed. Consider
switch to high dose
- Do not exceed 24mg total per
24hrs
ORDER:
- Buprenorphine 4mg or 8mg x1
- Schedule Buprenorphine 4mg
TID, first dose upon admission to
unit
- Buprenorphine 2mg q2hr PRN (3
doses max) CINA = 5 or greater
- Notify provider if CINA >5 after
1hr of 4mg total dose given OR if
there are concerns for precipitated
withdrawal*
- If notified, consider giving
additional 4-8mg with multiple
rounds, as needed. Consider
switch to high dose
- Do not exceed 24mg total per
24hrs
*precipitated withdrawal: patient feeling symptomatically
worse, unimproved with buprenorphine
Non-opioid medications to consider adding, though often not needed
- Methocarbamol 750mg or 1500mg PO Q6H PRN muscle spasm
- Naproxen 375mg PO Q8H PRN pain/muscle aches (do not order if
ibuprofen already ordered)
- Dicyclomine 20mg PO Q6H PRN abdominal cramps
- Clonidine 0.1mg PO Q4H PRN pulse>90, SBP>140, DBP>90
- Loperamide 4mg PO PRN at onset of diarrhea then 2mg after each
subsequent loose stool not to exceed 16mg total dose in 24 hours