Premenstrual Syndrome and Premenstrual Dysphoric Disorder Mind-Maps
•
0 likes•191 views

This document summarizes information about premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD), including their epidemiology, etiology, clinical presentation, diagnosis, and treatment options. Some key points include: 1) PMS affects up to 80% of women and involves cyclic symptoms in the last week of the menstrual cycle, while PMDD is more severe and affects 1.3-9% of women; 2) Both involve changes in hormone levels like progesterone and involve biological, psychological and social factors; 3) Diagnosis of PMDD requires 5 symptoms including mood changes that interfere with life and improve with menstruation. Treatment includes lifestyle changes, nutritional supplements, hormonal birth

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Premenstrual Syndrome and Premenstrual Dysphoric Disorder Mind-Maps
Similar to Premenstrual Syndrome and Premenstrual Dysphoric Disorder Mind-Maps (20)
More from Arwa M. Amin
More from Arwa M. Amin (20)
Recently uploaded
Recently uploaded (20)
Premenstrual Syndrome and Premenstrual Dysphoric Disorder Mind-Maps
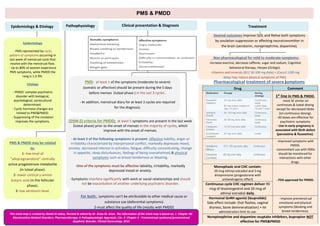
- 1. PMS & PMDD TreatmentPathophysiologyEpidemiology & Etiology Clinical presentation & Diagnosis Epidemiology - PMS represented by cyclic pattern of symptoms occurring in last week of menstrual cycle that resolve with the menstrual flow. - Up to 80% of women experience PMS symptoms, while PMDD the rang is 1.3-9%. Etiology - PMDD: complex psychiatric disorder with biological, psychological, sociocultural determinant. - Cyclic hormone changes are related to PMS&PMDD. - Suppressing of the ovulation improves the symptoms. Desired outcomes Improve QOL and Relive both symptoms by ovulation suppression or affecting neurotransmitter in the brain (serotonin, norepinephrine, dopamine). PMS & PMDD may be related to: 1- low level of "allopregnanolone” centrally active progesterone metabolite (in luteal phase). 2- lower cortical y-amino butyric acid (in the follicular phase). 3- low serotonin level. For both: symptoms can't be attributable to other medical cause or substance use (deferential symptoms) 2-must affect the quality of life (mostly with PMDD) This mind-map is created by Shahd Al-Johny. Revised & edited By Dr. Arwa M. Amin. The information of the mind-map is based on; 1- Chapter 96: Menstruation-Related Disorders, Pharmacotherapy: A Pathophysiologic Approach, 11e. 2- Chapter 2 - Premenstrual syndrome/premenstrual dysphoric disorder, Clinical Gynecology, 2015 (DSM-5) criteria for PMDD: at least 5 symptoms are present in the last week (luteal phase) prior to the onset of menses in the majority of cycles, which improve with the onset of menses. - At least 5 of the following symptoms is present: Affective liability, anger or irritability characterized by interpersonal conflict, markedly depresses mood, anxiety, decreased interest in activates, fatigue, difficulty concentrating, change in appetite, sleep disturbances, feelings of being overwhelmed,& physical symptoms such as breast tenderness or bloating. -One of the symptoms must be affective labiality, irritability, markedly depressed mood or anxiety. -Symptoms interfere significantly with work or social relationships and should not be exacerbation of another underlying psychiatric disorder. Pharmacological treatment of severe symptomsPMS: at least 1 of the symptoms (moderate to severe) (somatic or affective) should be present during the 5 days before menses (luteal phase ) in the last 3 cycles . - In addition, menstrual diary for at least 2 cycles are required for the diagnosis. Non pharmacological for mild to moderate symptoms: -Increase exercise, decrease caffeine, sugar and sodium, Cognitive behavioral therapy, Herpes (Ginkgo). -Vitamins and minerals (B12 50-100 mg daily) + (Caco3 1200 mg daily) may reduce physical symptoms of PMS. CommentDrug 1st line in PMS & PMDD. -most SE similar on continoues & luteal dosing except for decreased libido (on continuous dosing). -All doses are effective for psychiatric symptoms - Use in early pregnancy is associated with Birth defect (paroxetine & fluoxetine). -Improved symptoms with PMDD. -concomitant use with SSRIs should be monitored for interactions with other drugs. - FDA approved for PMDD. Monophasic oral CHC contain: 20 mcg ethinyl estradiol and 3 mg drospirenone (progesterone with antiandrogenic effect) Continuous cycle CHC regimen deliver 90 mcg of levonorgestrol and 20 mcg of ethinyl estradiol daily. - Improve premenstrual emotional and physical symptoms (bloating and breast tenderness). Hormonal GnRH agonist (leuprolide) Side effect include: (hot flashes, vaginal dryness, bone demineralization) + IM administration limit its use. Norepinephrine and dopamine reuptake inhibitors, bupropion NOT effective for PMS&PMDD
- 2. PMDD Defntion Sever form of PMS , 3-8% , not common, has an Official dignosis in mental disorders, may be misdiagnosed with bibolar. Criteria You need to have a total of 5 symptoms of 11 in the week befor period and improve within days of starting the period then become minimal or absent in the week after the period for most of the periods. Emotinal (Affective) Physical (Somatic) You must have 1 or more of: Mood swings, sudden sad, senestivty to rejection, irrtabilty, interpersonal conflict, depressed mood, hoplessness, putting your self down, anixity, tension, keyed up or edgy. You must have 1 or more of: Decresed intrest in usual activity, trubble conctrating, low energy, appetite change (increase or decrease), hypersomnia or insomnia, overwhelemd, breast tendenest, swelling, muscle pain, bloated Pathophysiligy Drop in progestrone level ( if the menstral cycle is 28 days, in the first 2 weeks a follicule in the ovart grows to an egg, egg is relased and leave behimd empty follicle "corpus lutim=yellow body" that secret progesterone to build the lining of the uterus, if the egg is not fertlized the corpus lutim disappear and progsterone drop that result in period ) Progestrone convert to allopregnalone that bind to GABAA receptors, so has effect of decreese anixity and depression. Dignosis - keep daily diart of symptoms for 2 mounth. – The official tool for screening for symptoms is called ( Daily recored of sevirtyof proplem ) Treatment Pharmacological Drug Dosing and comment SSRIs (paroxitine,sertraline, fluxitine are FDA approved) they acclerate conversion of progestrone to allopregnalol faster then increasing sertonin level to treat the depression. Intermittnt: start 7-10 befor period and stop once period is began, medication with short t12 like paroxitine increase the withdeowal symptoms, so start with minimal dose. Fluxtine have long t12. Continous: constant use of the drug ( if you have depressive symptoms between the periods). *Note: this may likely need to confirm the dignosis due to increase the risk of deprssion+PMDD ) Hormonal therapy : combination of ethinyl estradiol and drospirenone ( YAZ ) ( FDA approved for PMDD ). GnRH agonist: Leuprolide : it Stops production of estrogen and progestron. ( medical (Chemical) menupouse). *Side Effect of menupuse symptoms: hot flashes, night sweeting. Non pharmacological Diet: Lifestyle Nutrtinal supplemnt Herpes Light therapy Decrease sugar, caffiene, soduim, nicotine, alcohol. Sleep 7-9 hours Regular Exersise 3-5 days a week - Calsuim 1200 mgday. - Vit B6 50-100 mgday. " dose < 100 can cause perphial nuoropathy. - MG 200-360 mgday. - Vit E 400Uday. Agnus castus= chastberry. -Ginko biloba. Need more studies )Watch This by Dr. Tracey Marks-If You Suffer from Premenstrual Dysphoria(ofVideo SUMMARY Summary by Shahd Al-Johny. Revised & edited By Dr. Arwa M. Amin . Reference: YouTube video: If You Suffer from Premenstrual Dysphoria - Watch This by Dr. Tracey Marks