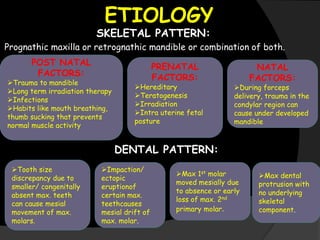
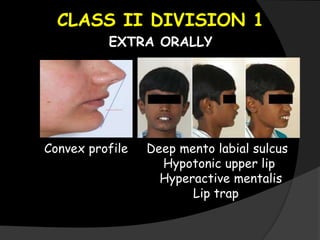
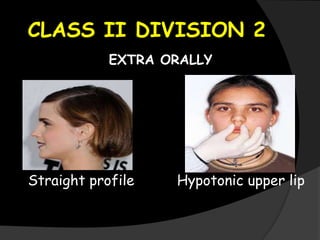
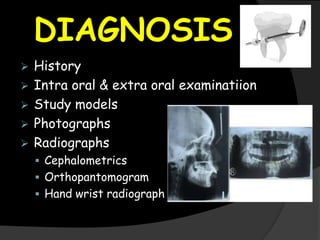
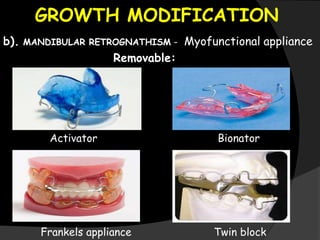
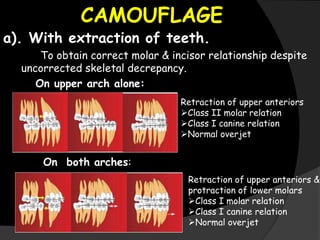
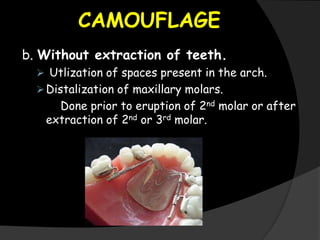
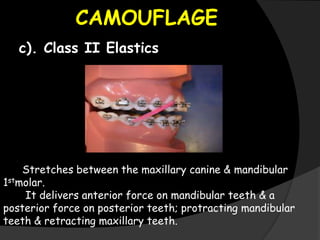
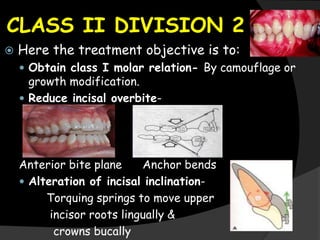
This document discusses the classification, etiology, clinical features, diagnosis, and management of Class II malocclusions. It describes two main types, Class II division 1 characterized by a distally placed mandible and Class II division 2 by a protruded maxilla. Etiology may include hereditary factors or trauma influencing jaw growth. Clinical features and intraoral examination are used for diagnosis. Management approaches include growth modification using headgear or myofunctional appliances, camouflage treatment using extractions or elastics, or in severe cases, jaw surgery.