Download as PDF, PPTX










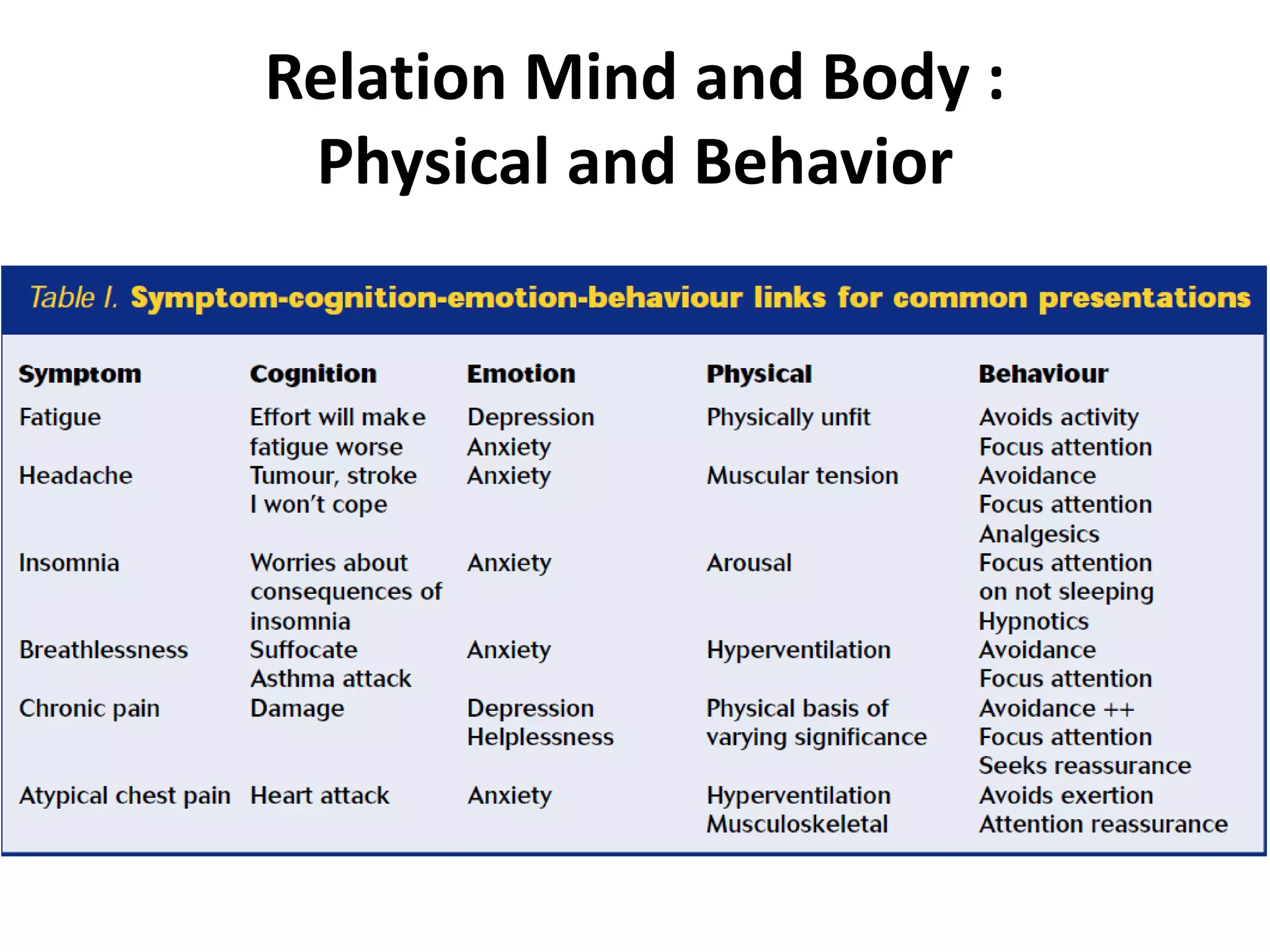












Dr. Andri, a psychiatrist and fellow of the Academy of Psychosomatic Medicine, presents on psychosomatic disorders, emphasizing the mind-body connection and the historical evolution of related diagnoses in DSM. He highlights the prevalence of somatic symptoms in clinical practice, often leading to misdiagnosis or overlooked psychiatric conditions, and proposes treatment strategies that incorporate both pharmacological and non-pharmacological approaches. Key insights include the importance of understanding patients' symptoms, establishing a therapeutic alliance, and the need for interdisciplinary management of somatic symptom disorders.































































































