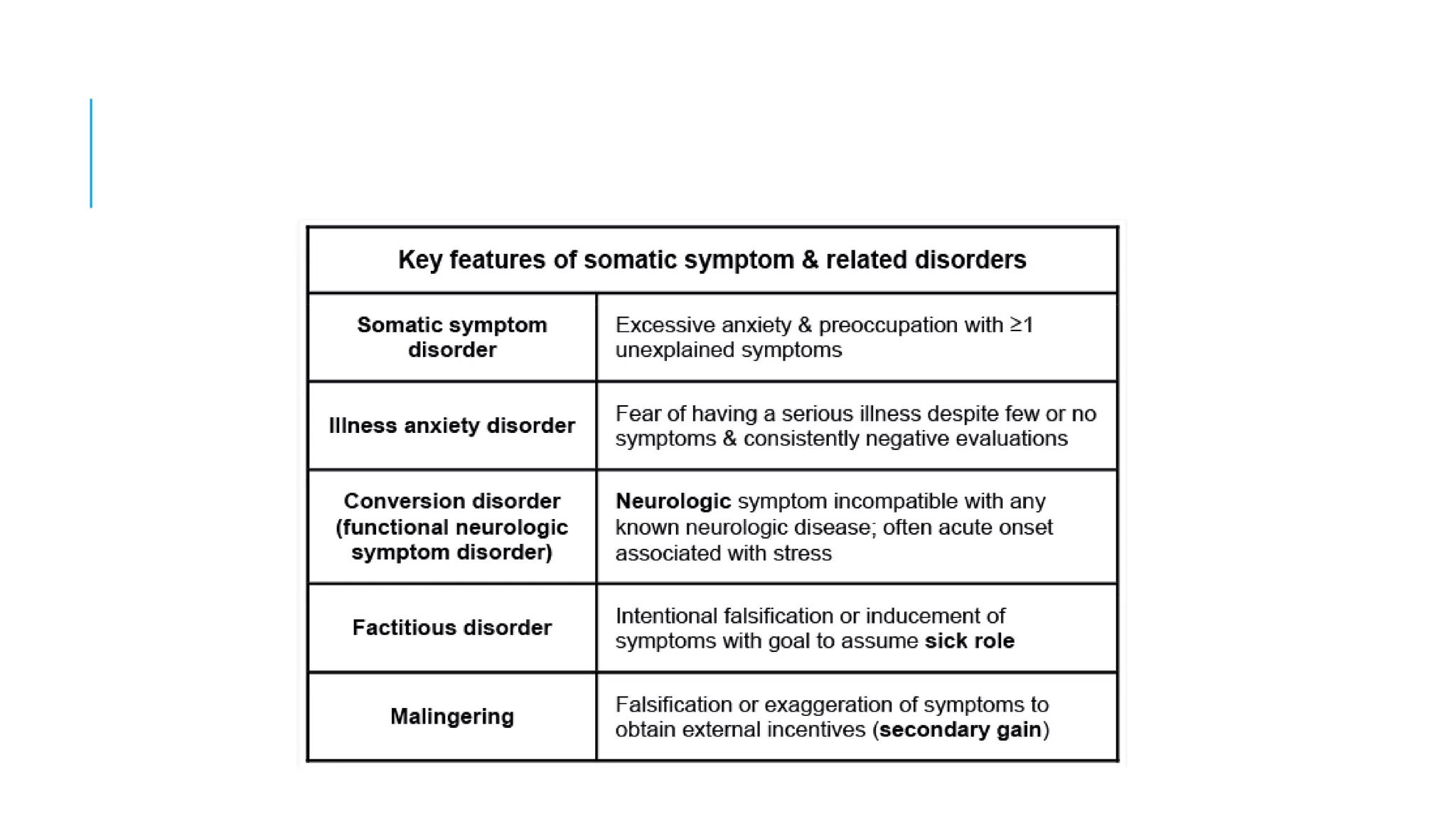
This document discusses somatic symptom and related disorders. It defines psychological factors that can affect medical conditions by exacerbating symptoms or interfering with treatment. It provides qualifiers to describe the severity of these psychological influences. The key features and differential diagnosis of various somatic symptom disorders are outlined, including somatic symptom disorder, illness anxiety disorder, and factitious disorders. Screening tools like the PHQ-15 and SSS-8 are presented. Treatment approaches are emphasized, including scheduling regular appointments, educating patients, evaluating somatic symptoms, treating comorbid conditions, and using cognitive behavioral therapy and medication.













![Somatic Symptom Scale – 8 [SSS-8]](https://image.slidesharecdn.com/somaticsymptomandrelateddisorder-190331111326/75/Somatic-symptom-and-related-disorder-19-2048.jpg)







![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)















![Organic Brain Syndromes [2002]](https://cdn.slidesharecdn.com/ss_thumbnails/organicmentaldisorders-171116041412-thumbnail.jpg?width=640&height=640&fit=bounds)
















































