
Recommended
More Related Content
What's hot
What's hot (20)
Similar to HYPOSPADIAS & EPISPADIAS.pptx
Similar to HYPOSPADIAS & EPISPADIAS.pptx (20)
More from AminaRajah1
Recently uploaded
Recently uploaded (20)
HYPOSPADIAS & EPISPADIAS.pptx
- 1. EPISPADIAS & HYPOSPADIAS BY RAJAH AMINA SULEIMAN (RN, RM, RNE, RBPN, BNSC, PGDE, MSC)
- 6. HYPOSPADIAS
- 7. INTRODUCTION Hypospadias is one of the most common, complex and diverse urologic anomalies encountered in children. Hypospadias is a birth defect in boys where the opening of the urethra is not located at the tip of the penis. Hypospadias is one of the most common congenital anomalies in men. In boys with hypospadias, the urethra forms abnormally during weeks 8–14 of pregnancy. The abnormal opening can form anywhere from just below the end of the penis to the scrotum.
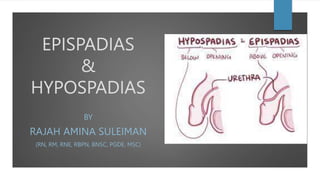
- 8. DEFINITION Hypospadias is an abnormality of anterior urethral and penile development, in which the urethral opening is ectopically located on the ventral aspect of the penis proximal to the tip of the glans penis. OR Hypospadias is a congenital abnormality of the penis that is characterized by an abnormal position of the urethral opening. OR Hypospadias is a congenital defect causing the urethral meatus to be located at an abnormal site, usually on the underside of the penis rather than at the tip.
- 9. INCIDENCE Hypospadias is the second most common genital birth defect in boys, following cryptorchidism. With an incidence of 1 in 300 live male births worldwide.
- 10. ETIOLOGY The cause of hypospadias is a mix of monogenic and multifactorial forms, implicating both genes and environmental factors.
- 11. RISK FACTORS Age : Mothers who were age 35 years or older had a higher risk of having a baby with hypospadias Weight: Mothers who were considered obese had a higher risk of having a baby with hypospadias Fertility treatments: Women who used assisted reproductive technology to help with pregnancy had a higher risk of having a baby with hypospadias Certain hormones: Women who took certain hormones just before or during pregnancy were shown to have a higher risk of having a baby with hypospadias
- 12. CLASSIFICATION
- 13. FEMALE HYPOSPADIAS In contrast to male hypospadias, female hypospadias (FH) or “hypospadia feminis” is such a rare anomaly of the lower urogenital system that most textbooks fail even to mention it. Isolated Female Hypospadias, with no associated genitourinary abnormalities, is even rarer.
- 14. PATHOPHYSIOLOGY Hypospadias is a congenital abnormality of the penis characterized by an abnormal position of the urethral opening that occurs during the embryologic development of the urethra, between 8 and 20 weeks' gestation. Males and females have identical external genital structures until 8 weeks, after which the genital structures develop a masculine phenotype in males, primarily under the influence of testosterone and its byproduct, dihydrotestosterone. Under the influence of these hormones, the genital tubercle becomes rapidly elongated, forming the phallus, whereas the urethral folds are pulled by the phallus to form the lateral walls of the urethral groove.
- 15. PATHOPHYSIOLOGY The urethral folds coalesce in the midline from base to tip, forming a tubularized penile urethra and median scrotal raphe. The endoderm differentiates to ectoderm with subsequent canalization by apoptosis. The prepuce normally forms as a ridge of skin from the corona that grows circumferentially, fusing with the glans. Failure of fusion of the urethral folds in hypospadias impedes this process, and a dorsal hooded prepuce results. Ventral curvature of the penis, termed chordee, is often associated with hypospadias, especially in more severe forms. Hypospadias occurs due to arrest of penile development, leading to hypoplasia of the ventral tissue of the penis.
- 16. CLINICAL MANIFESTATIONS OF HYPOSPADIAS There are 3 key features of hypospadias, although not all 3 are required for the condition: 1) Ventral opening of the urethral meatus 2) Ventral curvature of the penis or “Chordee” 3) Dorsal hooded foreskin Others Include: Abnormal spraying of urine Cryptorchidism (undescended testes)
- 17. DIAGNOSIS Hypospadias is usually diagnosed during a physical examination after the baby is born.
- 18. SURGICAL MANAGEMENT Timing: Surgical intervention for hypospadias can be performed at any age, however, The American Academy of Pediatrics recommend operative intervention at 6–18 months, to limit psychological stress and subsequent behavioural problems seen in toddlers undergoing genital surgery. NOTE: It is recommended that patients with hypospadias should not be circumcised because of the superiority of the prepuce tissue covering the urethra.
- 19. SURGICAL MANAGEMENT The operative steps of hypospadias surgery involve: Penile Degloving Correction of Ventral Chordae (orthoplasty or penile straightening) Reconstruction of the urethra (urethroplasty) Providing a vascularized coverage for the urethroplasty Reconstruction of the glans (glansplasty) Meatoplasty and Glanuloplasty Scrotoplasty Cosmetic skin coverage to create a circumcised penile appearance.
- 20. POST-OPERATIVE COMPLICATIONS Urethrocutaneous fistula Meatal stenosis Urethral stenosis Glans dehiscence Urethral diverticulum or urethrocele, which can lead to infections and post-void dribbling Cosmetic issues: Excess residual skin, skin tags, inclusion cysts, skin bridges, suture tracts Hair-bearing urethra Recurrent or persistent penile curvature Spraying or misdirected urinary stream and/or irritative symptoms Erectile dysfunction Balanitis xerotica obliterans of the urethra leading to strictures
- 21. NURSING MANAGEMENT PRE-OPERATIVE MANAGEMENT Admission History and physical examination Observations: v/signs Pre-operative Investigations: FBC, FBS, Hb, PCV, X-rays, HIV, Hep, Bleeding and clotting time, Coagulation tests etc Nutrition: NPO at least 6 hrs Physical care Psychological care
- 22. NURSING MANAGEMENT PRE-OPERATIVE MANAGEMENT Informed consent Pre-surgical medications: sedatives Clinical Photograph Counselling
- 23. NURSING MANAGEMENT POST-OPERATIVE MANAGEMENT Preparation to receive the patient Reception Pain relief: Analgesia should be prescribed to be taken preemptively, particularly for the first 72 hours, when the inflammatory phase is expected to begin abating. Psychological care Clinical photograph
- 24. NURSING MANAGEMENT POST-OPERATIVE MANAGEMENT Wound care including drains, bandaging Medications Fluid intake Health education Input and Output chart: Notify the surgeon if there is no urine drainage for 1 hour as this may indicate kinks in the system or obstruction by sediment. Discharge Follow up
- 25. EPISPADIAS
- 26. INTRODUCTION Epispadias is a rare congenital malformation of the male or female urogenital organs that consists of a defect of the dorsal wall of the urethra. In boys with epispadias, the urethra generally opens on the top or side of the penis rather than the tip. However, it is possible for the urethra to be open along the entire length of the penis. In girls, the opening is usually between the clitoris and the labia but may be in the abdominal area. Epispadias can be associated with bladder exstrophy.
- 27. DEFINITION Epispadias is a rare urogenital malformation characterized by the failure of the urethral tube to tubularize on the dorsal aspect. Epispadias is an abnormality of the urethra in which the urethral opening is ectopically located on the dorsal aspect of the penis.
- 29. INCIDENCE Epispadias occurs in one in 117,000 newborn boys one in 484,000 newborn girls. It is commonly seen as a component in the spectrum of bladder exstrophyepispadias- complex (BEEC). Isolated epispadias constitutes less than 10 percent of the total cases of epispadias. Isolated male epispadias is rare.
- 30. ETIOLOGY Epispadias can be explained by defective migration of the paired primordia of the genital tubercle that fuse on the midline to form the genital tubercle at the fifth week of embryologic development. Epispadias is rarely observed in 2 members of the same family.
- 31. CLASSIFICATION Glandular Penile Complete (ie, penopubic).
- 32. FEMALE EPISPADIAS Isolated female epispadias without bladder exstrophy is an extremely rare congenital anomaly. The symptoms of female epispadias are primary urinary incontinence and abnormal anatomical features. In females, epispadias consists of bifid clitoris with diastases of the corpora cavernosa, flattening of the mons, and separation of the labia.
- 33. CLINICAL MANIFESTATION (MALE) Abnormal opening from the joint between the pubic bones to the area above the tip of the penis Backward flow of urine into the kidney (reflux nephropathy) Short, widened penis with an abnormal curvature Urinary tract infections Widened pubic bone
- 35. CLINICAL MANIFESTATION (FEMALE) Abnormal clitoris and labia Abnormal opening from the bladder neck to the area above the normal urethral opening Backward flow of urine into the kidney (reflux nephropathy) Widened pubic bone Urinary incontinence Urinary tract infections
- 36. DIAGNOSIS Physical Examination Blood test to check electrolyte levels Intravenous pyelogram (IVP), a special X-ray of the kidneys, bladder and ureters MRI and CT scans, depending on the condition Pelvic X-ray Ultrasound of the urogenital system
- 37. SURGICAL MANAGEMENT Surgical management of epispadias is challenging and requires technical expertise. The surgery aims to reconstruct the genitalia and urethra, providing optimal functional and cosmetic outcomes. At present, surgeons across the world have adopted either of the two following approaches: Modified Cantwell-Ransley repair Complete penile disassembly technique (Mitchell and Bagli)
- 38. NURSING MANAGEMENT Assess the newborns flow of urine, exit site, and angle of urination Infant/child returns from surgery w/ penis wrapped in a simple dressing and a stent or catheter for urinary drainage Fresh blood may be seen on the dressing and in the stent or catheter in the immediate postop period, but the urine should become less bloody over the next few hours Encourage fluid intake to maintain adequate urinary output and patency of the stent
- 39. NURSING MANAGEMENT Accurate hourly Input & output is essential Notify HCP if no urine drainage for 1 hour Once caudal block wears off, acetaminophen or ibuprofen should be administered for pain as ordered Antibiotics are usually prescribed until the urinary stent falls out or is removed Double diapering protects the stent
- 40. COMPLICATIONS Wound infection Dysuria (due to bladder spasms) Urethral stricture and obstruction Persistent chordee Persistent short length Urethral retraction and hypospadias Partial or complete penile loss
- 41. THANK YOU FOR LISTENING ANY QUESTIONS?
Editor's Notes
- FIGURE 55: THE MALE REPRODUCTIVE SYSTEM 1. Vas Deferens 2. Bladder 3. Prostate gland 4. Urethra 5. Glans penis 6. Epididymis 7. Scrotum 8. Testis 9. Seminal vesicle 10. Colon
- The penis consists of 3 parts including the base, shaft (body or corpus), and glans. The shaft is made from 3 columns of erectile tissue: the left and right corpora cavernosa and the corpus spongiosum, which are all innervated by the parasympathetic fibers of the pelvic splanchnic nerves