
Recommended
More Related Content
What's hot
Similar to Hemostasis work up
Similar to Hemostasis work up (20)
More from AbdulKaderSouid
More from AbdulKaderSouid (13)
Recently uploaded
Recently uploaded (20)
Hemostasis work up
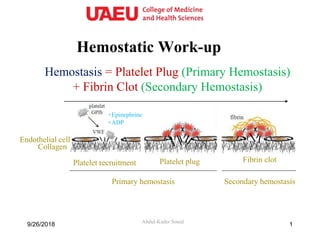
- 1. Hemostatic Work-up Abdul-Kader Souid Hemostasis = Platelet Plug (Primary Hemostasis) + Fibrin Clot (Secondary Hemostasis) Collagen Endothelial cell Platelet recruitment Platelet plug Fibrin clot Primary hemostasis Secondary hemostasis +ADP +Epinephrine 9/26/2018 1
- 2. Primary Hemostasis 2 Primary hemostasis work-up • Platelet count • Platelet function screen • vWF antigen & activity 9/26/2018 Platelet Plug = Platelets + vWF The three main functions of von Willebrand factor (vWF) 3) Factor VIII delivery 1) Platelet adhesion to collagen 2) Platelet-platelet spreading and aggregation Collagen vWF GPIb-a Platelet GPIIb/IIIa vWF Fibrinogen Platelet Factor VIII Must know
- 3. Platelet Function Screen The instrument measures the time taken for blood pulled through a fine capillary to block a membrane coated with collagen-ADP or collagen-epinephrine. 39/26/2018 Blood Capillary tube Coated membrane Platelet Function Analyzer (PFA100) Must know
- 4. Platelet Function Screen • Normal vWF and platelet function = Collagen-epinephrine <164 sec + collagen-ADP <116 sec • Abnormal vWF (common) or abnormal platelet function (rare) = Collagen-epinephrine >164 sec + collagen-ADP >116 sec • Aspirin & NSAID (common) = Collagen-epinephrine >164 sec + collagen-ADP <116 sec 9/26/2018 4 Blood Capillary tube Coated membrane Must know
- 5. Secondary Hemostasis 59/26/2018 Work-up PT/INR aPTT TT Fibrinogen TFPI = Tissue factor pathway inhibitor prothrombin thrombin (IIa) fibrinogen fibrin prothrombinase complex (X, V, PL, Ca2+ ) tissue factorVII IX XI VIII IIa TFPI Cross-over reaction ExtrinsicCascade IntrinsicCascadeCommonCascade Must know
- 6. Secondary Hemostasis • Prothrombin time (PT/INR): – Citrated plasma + Ca2+ + phospholipid + tissue factor → √ the time to clot – Sensitive to factors I, II, V, VII, X (extrinsic & common pathways). – International normalized ratio (INR) = – ISI (International Sensitivity Index) = 1.0 to 2.0 (reflects tissue factor activity) • Activated Partial thromboplastin time (aPTT): – Citrated plasma + Ca2+ + phospholipid + silica → √ the time to clot – Sensitive to factors I, II, V, VIII, IX, X, XI, XII (intrinsic & common pathways). • Thrombin time (TT): – Citrated plasma + Ca2+ + phospholipid + thrombin → √ the time to clot – Sensitive to factor I (fibrinogen) and heparin (anti-thrombin). 69/26/2018 Must know
- 7. ↑Thrombin Time (↑TT) aPTT 55.6 sec (normal, 35.2 - 40.4), PT 23.2 sec (normal, 12.2 - 14.6), TT 21.4 sec (normal, 9.2 - 12.3) PTPTT TTprothrombin thrombin (IIa) fibrinogen fibrin prothrombinase complex (X, V, PL, Ca2+ ) tissue factorVII IX XI VIII XII 7 ↑Thrombin time (TT) = ↓Fibrinogen (hypofibrinogenemia) or presence of heparin 9/26/2018 Must know
- 8. ↑Prothrombin Time (↑PT) aPTT 35.6 sec (normal, 35.2 - 40.4), PT 23.2 sec (normal, 12.2 - 14.6), TT 11.4 sec (normal, 9.2 - 12.3). PTPTT TTprothrombin thrombin (IIa) fibrinogen fibrin prothrombinase complex (X, V, PL, Ca2+ ) tissue factorVII IX XI VIII XII 8 ↑PT with normal aPTT and TT = factor VII deficiency 9/26/2018 Must know
- 9. ↑aPTT aPTT 75.6 sec (normal, 35.2 - 40.4), PT 13.2 sec (normal, 12.2 - 14.6), TT 11.4 sec (normal, 9.2 - 12.3). PTPTT TTprothrombin thrombin (IIa) fibrinogen fibrin prothrombinase complex (X, V, PL, Ca2+ ) tissue factorVII IX XI VIII XII 9 ↑aPTT with normal PT and TT = factor XII, XI, IX, or VIII deficiency 9/26/2018 Must know
- 10. A 10-year-old healthy boy with ↑aPTT on a pre-op testing ↑aPTT, corrected with 1:1 mixing of patient plasma with normal plasma + ↓factor XII → Factor XII deficiency (clinically insignificant). Must know Note: ↑aPTT due to anti-phospholipid antibodies do not correct with the mixing study. These antibodies do not cause bleeding and the prolonged aPTT would be clinically insignificant. Two Limitations of the aPTT Test
- 11. aPTT 75.6 sec (normal, 35.2 - 40.4), PT 32.2 sec (normal, 12.2 - 14.6), TT 11.4 sec (normal, 9.2 - 12.3). PTPTT TTprothrombin thrombin (IIa) fibrinogen fibrin prothrombinase complex (X, V, PL, Ca2+ ) tissue factorVII IX XI VIII XII 11 ↑PTT and ↑PT with normal TT = factor II, V, or X deficiency (e.g., vitamin K deficiency which ↓factors II, VII, IX, & X) 9/26/2018 Must know ↑aPTT & ↑PT
- 12. Hemostatic Evaluation • Detailed bleeding history • Platelet count • Platelet function screen • vWF antigen (vWf:Ag) and activity (vWf R:Co) • Blood group • aPTT, PT/INR, TT 9/26/2018 12
- 13. a) Factor VIII deficiency b) NSAID c) Vitamin K deficiency d) von Willebrand disease e) Hypofibrinogenemia f) Factor VII deficiency 1. ↑Collagen-epinephrine + ↑Collagen-ADP 2. ↑Collagen-epinephrine + nl Collagen-ADP 3. ↑aPTT, nl PT, nl TT 4. aPTT, ↑PT, nl TT 5. ↑aPTT, ↑ PT, ↑TT 6. ↑aPTT, ↑ PT, nl TT “Must Know Pearls” 9/26/2018 13
- 14. Q. A 22-year-old female patient is diagnosed with vitamin K deficiency. Which of the following is the most likely finding on her hemostatic evaluation? A. ↑PT, ↑aPTT, nl TT B. nl PT, ↑aPTT, nl TT C. ↑PT, nl aPTT, nl TT D. ↑PT, ↑aPTT, ↑TT 149/26/2018
- 15. 9/26/2018 15 A 23-year-old patient presents to the clinic for menorrhagia. Her evaluation reveals a normal platelet count, thrombin time (TT), prothrombin time (PT), activated partial thromboplastin time (aPTT), von Willebrand factor antigen and activity, and platelet function screen. Her older sister has a history of heavy menstrual bleeding and delayed postpartum bleeding. Further testing shows increased fibrinolysis. Which one of the following laboratory findings is most likely to be found in this patient? A. Decreased plasminogen B. Decreased plasminogen activator inhibitor-1 (PAI-1) C. Increased α2-antiplasmin D. Increased thrombin-activatable fibrinolysis inhibitor (TAFI) E. Decreased tissue factor pathway inhibitor (TFPI)
- 16. Comments This patient has menorrhagia and ↑ fibrinolysis due to ↓ “plasminogen activator inhibitor-1” (PAI-1). ↓Plasminogen, ↑α2-antiplasmin, ↑thrombin-activatable fibrinolysis inhibitor (TAFI), and ↓TFPI are not associated with bleeding. Plasminogen plays an important role in fibrinolysis; it is converted to plasmin, which converts fibrin into fibrin degradation products (FDPs). Activators of plasminogen are tissue plasminogen activator (tPA) and urokinase plasminogen activator. Inhibitors of plasminogen are PAI- 1, which regulates tPA and urokinase plasminogen activator, and α2-antiplasmin. Thrombin-activatable fibrinolysis inhibitor (TAFI) inhibits the conversion of fibrin to FDPs. PAI-1 deficiency is autosomal recessive (OMIM#173360; serpine1, serpin peptidase inhibitor, clade e (nexin, plasminogen activator inhibitor type 1), member 1). A complete deficiency of PAI-1 is associated with mild-to-moderate mucocutaneous bleeding. The diagnosis is made by measuring PAI-1 activity and antigen and detecting mutations in SERPINE1. Treatment is plasma + antifibrinolytics (aminocaproic acid, tranexamic acid). Furie B, Furie BC. Mechanisms of thrombus formation. N Engl J Med. 2008; 359(9):938-949. Heiman M, Gupta S, Khan SS, Vaughan DE, Shapiro AD. Complete plasminogen activator inhibitor 1 deficiency. GeneReviews. PMID: 28771291 Rijken DC, Lijnen HR. New insights into the molecular mechanisms of the fibrinolytic system. J Thromb Haemost. 2009;7:4-13.
- 17. 9/26/2018 17