
Recommended
More Related Content
What's hot
What's hot (20)
Similar to von willebrand disease.ppt
Similar to von willebrand disease.ppt (20)
More from AbdulKaderSouid
More from AbdulKaderSouid (12)
Recently uploaded
Recently uploaded (20)
von willebrand disease.ppt
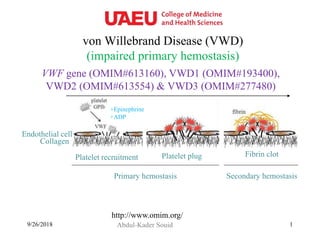
- 1. von Willebrand Disease (VWD) (impaired primary hemostasis) Abdul-Kader Souid9/26/2018 1 Collagen Endothelial cell Platelet recruitment Platelet plug Fibrin clot Primary hemostasis Secondary hemostasis +ADP +Epinephrine http://www.omim.org/ VWF gene (OMIM#613160), VWD1 (OMIM#193400), VWD2 (OMIM#613554) & VWD3 (OMIM#277480)
- 2. 9/26/2018 2
- 3. 9/26/2018 3
- 4. von Willebrand Factor (VWF) • This multimeric glycoprotein is found in plasma, platelet α-granules, and subendothelial tissue. • It binds to GP1b receptors on platelet surface to form bridges between platelets and collagen in areas of vascular damage. • The RGD (Arg-Gly-Asp) motif of VWF bridges between thrombin-activated platelets via the fibrinogen receptors GPIIb/IIIa, forming platelet plugs. • VWF also binds and stabilizes factor VIII. – Severe deficiency (or absence) of VWF causes secondary deficiency of factor VIII. • Deficiency of VWF results in defective platelet adhesion (impaired primary hemostasis). Deficiency of GPIb → Bernard–Soulier syndrome Deficiency of GPIIb/IIIa → Glanzmann thrombasthenia 3) Factor VIII delivery 1) Platelet adhesion to collagen 2) Platelet-platelet spreading and aggregation Collagen vWF GPIb-a Platelet GPIIb/IIIa vWF Fibrinogen Platelet Factor VIII Must know Ristocetin causes in vitro platelet aggregation in the presence of VWF.
- 5. Platelet activation by ADP (blocked by clopidogrel) causes conformational changes in platelet GPIIb/IIIa (integrin αIIbβ3) receptors that induce binding to fibrinogen. 9/26/2018 5 3) Factor VIII delivery 1) Platelet adhesion to collagen 2) Platelet-platelet spreading and aggregation Collagen vWF GPI b- a Platelet GPIIb/IIIa vWF Fibrinogen Platelet Factor VIII Deficiency of GPIIb/IIIa → Glanzmann Thrombasthenia Understanding of the role of GpIIb/IIIa (integrin αIIbβ3) in Glanzmann thrombasthenia led to the development of GpIIb/IIIa inhibitors, a class of powerful antiplatelet agents (e.g., abciximab, eptifibatide, tirofiban). Must know
- 6. Hemostatic Work-up: • Platelet count • ABO blood group – Individuals with blood type O have 25% less VWF) • Platelet function screen • VWF antigen (VWF:Ag) • VWF activity – R:CoF; ristocetin co-factor activity • aPTT, PT/INR, TT • Factor VIII activity – Typically normal 9/26/2018 6 Clinical Presentations: • Recurrent epistaxis • Menorrhagia • Bleeding post tonsillectomy or dental extraction Must know
- 8. VWD: Treatment • The treatment of choice is “desmopressin + tranexamic acid”. • The recently approved (December 08, 2015) recombinant VWF (rVWF, vonicog alfa, Vonvendi) is reserved for patients with R:CoF levels <10 U/dL or with severe bleeding. – The rVWF dose for minor bleeding is 40-50 IU/kg, repeated every 8-24 h as needed clinically. – The rVWF for major bleeding is 50-80 IU/kg, followed by 40- 60 IU/Kg every 8-24 h for 2-3 days as needed clinically. – When using rVWF, it is recommended that rFVIII be given within 10 min of the first dose of rVWF. – The antifibrinolytic agent tranexamic acid is also recommended. Must know Up-to-Date - Nov 27, 2017
- 9. (1) Aminocaproic acid (Amicar; DrugBank name DB04134), not available in the UAE. 9/26/2018 9 Fibrinolytic inhibitors for Mucosal Bleeding (2) Tranexamic Acid (DB00302); available in the UAE. Must know (halt fibrinolysis by inhibiting plasminogen & plasmin) http://www.drugbank.ca/ The antifibrinolytic drugs are indicated for mucosal bleeding due to factor VIII, factor IX, or vWF deficiency. The World Federation of Hemophilia guidelines recommend oral tranexamic acid (1 g/dose or 10 mg/kg per dose 3 times daily) or aminocaproic acid (50 mg/kg 4 times daily with a maximum dose of 24 g daily) the day before dental surgery and then for a total of 7 days. “Fibrin glue” (fibrinogen + thrombin) is also used for local hemostasis during dental procedures.
- 10. • Desmopressin acetate (1-deamino-8-d-arginine vasopressin, or DDAVP) is the treatment of choice for mild-to-moderate factor VIII deficiency with minor bleeding. • It ↑factor VIII (and von Willebrand factor) level by 3-5 fold within 30 to 60 min of administration. • IV desmopressin (DDAVP Injection) is given at 0.3 g/kg in 50 mL of 0.9% NaCl over 30 min. • Intranasal desmopressin [Stimate Nasal Spray, one (150 g) or two (300 g) puffs] is equally effective. Desmopressin: Only for Factor VIII or VWF Deficiency Vasopressin Phe Gln NH2-Cys-S-S-Cys-Pro-L-Arg-Gly-NH2 Tyr Asn AsnTyr Cys-S-S-Cys-Pro-D-Arg-Gly-NH2 GlnPhe DDAVP [1-(deamino)-8-D-arginine vasopressin 9/26/2018 10 Must know Desmopressin is only indicated for mucosal bleeding due to factor VIII or VWF deficiency. A synthetic analog of vasopressin
- 11. Required Reading • American Society of Hematology. Evaluation and management of von Willebrand disease. American Society of Hematology website. http://ashpocketguides.hematology.org/#/app/guides/2/pages/ • Mannucci PM, Kempton C, Millar C, et al. Pharmacokinetics and safety of a novel recombinant human von Willebrand factor manufactured with a plasma-free method: a prospective clinical trial. Blood 2013;122:648. • James PD, Lillicrap D. von Willebrand disease: clinical and laboratory lessons learned from the large von Willebrand disease studies. Am J Hematol. 2012;87, Suppl 1:S4-S11. • Tosetto A, Castaman G. How I treat type 2 variant forms of von Willebrand disease. Blood 2015;125:907-914. • Nichols WL, et al. Von Willebrand disease (VWD): evidence-based diagnosis and management guidelines, the National Heart, Lung, and Blood Institute (NHLBI) Expert Panel report (USA). Haemophilia 2008;14:171-232. 9/26/2018 11
- 12. A 16-year-old female presents to the clinic with severe menorrhagia. Her hemoglobin is 104 g/L, platelet count 196 x109/L, aPTT 35.6 sec (normal, 35.2 - 40.4), PT 13.2 sec (normal, 12.2 - 14.6), INR 1.0 (normal, 0.8-1.2), and TT 11.4 sec (normal, 9.2 - 12.3). Collagen-epinephrine channel closure time is 201 sec (normal, ≤168) and collagen-ADP 138 sec (normal, ≤116). Which one of the following diagnoses is correct? A. von Willebrand disease B. Hemophilia A C. Hemophilia B D. Glanzmann thrombasthenia E. Bernard–Soulier syndrome
- 13. 9/26/2018 13 A 23-year-old patient presents to the clinic for menorrhagia. Her evaluation reveals a normal platelet count, thrombin time (TT), prothrombin time (PT), activated partial thromboplastin time (aPTT), von Willebrand factor antigen and activity, and platelet function screen. Her older sister has a history of heavy menstrual bleeding and delayed postpartum bleeding. Further testing shows increased fibrinolysis. Which one of the following laboratory findings is most likely to be found in this patient? A. Decreased plasminogen B. Decreased plasminogen activator inhibitor-1 (PAI-1) C. Increased α2-antiplasmin D. Increased thrombin-activatable fibrinolysis inhibitor (TAFI) E. Decreased tissue factor pathway inhibitor (TFPI)
- 14. VWD Classification • Type I (85% of cases, OMIM#193400): – Partial quantitative deficiency (levels 30-50%) – Normal vWf structure and functions – Autosomal dominant • Type II (15% of cases; autosomal dominant/recessive qualitative defect of VWF; OMIM#613554): – A (12%), absent high- and intermediate-weight (HMW) multimers and low VWF R:Co (loss-of-function). – B (3%), absent HMW multimers, ↑affinity of VWF for GP Ib (gain-of-function), thrombocytopenia; ↑aggregation to low-dose ristocetin. – M (rare), normal HMW multimers and low VWF R:Co. – N (Normandy, rare), normal vWf:Ag and VWF R:Co and decreased factor VIII level due to abnormal vWf structure. • Type III (nonsense mutations and gene deletion) - rare Optional
- 16. 9/26/2018 16 Laboratory tests for von Willebrand disease CBC, PT/INR, aPTT, TT, factor VIII These tests are typically normal. PTT may be elevated in severe VWD due to ↓factor VIII. Blood type Individuals with blood type O have 25% less VWF. Platelet Function Screen (PFA-100) Measures primary hemostasis. The instrument determines the time taken for blood forced through a fine capillary tube to block a membrane coated with collagen-epinephrine or collagen-ADP. Normal closure time for the collagen-epinephrine channel is <164 sec and for the collagen-ADP channel <116 s. In VWD or platelet dysfunction, the closure time for the collagen-epinephrine channel is >164 s and for the collagen-ADP channel >116 s. In Aspirin or NSAID, closure time for the collagen-epinephrine channel is >164 s and for the collagen-ADP channel <116 s. Ristocetin co- factor (vWf R:Co) and vWf antigen The most sensitive tests for VWD. Ristocetin (a positively charged antibiotic) activates VWF, causing its binding to platelets. The assays should be performed within 2 h of the venipuncture; otherwise, the plasma must be removed immediately and stored at - 70oC. Optional