Basic Mechanisms of Membrane Transport
•Download as PPTX, PDF•
0 likes•212 views

'Basic mechanisms of membrane transport is the topic of general pharmacology. Introduction- Membrane Transport Plasma Membrane Lipid solubility in membrane permeation Transporters Versus Channels Mechanisms of Transport Passive Diffusion Relationship between Molecular weight and Diffusion Carrier mediated Transport Facilitated Diffusion Active Transport Primary Active Transport P type- Na+ K+-ATPase Secondary Active transport- Symport, Antiport Intestinal Transporters with e.g Vesicular Transport-Exocytosis, Endocytosis-Phagocytosis,Pinocytosis Pore (Convective) Transport Ion Pair Formation

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Basic Mechanisms of Membrane Transport
Similar to Basic Mechanisms of Membrane Transport (20)
More from Akash Agnihotri
More from Akash Agnihotri (14)
Recently uploaded
Recently uploaded (20)
Basic Mechanisms of Membrane Transport
- 1. Basic Mechanisms of Membrane Transport Presenter- Akash Agnihotri
- 2. Introduction- Membrane Transport Transportation of molecules through plasma membrane/cell membrane Why we need transport ? Cells need Nutrients (Extracellular space) Cells need to get away (Toxic materials) Membrane transport proteins are present in all organisms Which controls – Influx- Essential nutrients & ions Efflux- Cellular waste, Environmental toxins, drugs & Xenobiotics etc 2
- 3. Plasma Membrane 3 Fluid Mosaic Model (Singer and Nicolson, 1972) 2 Types of pore- - 10nm - 50-70nm Pores provide channel- Water, ions & dissolved solutes (Urea) may move (Pratt & Tylor 1990) Hydrophobic tails Hydrophilic Heads Phospholipid Bilayer
- 4. 4 Lipid solubility in membrane permeation Figures The importance of lipid solubility in membrane permeation Lipid solubility Membrane concentration CM
- 5. Transporters Versus Channels Channels In general, channels have two primary states, open and closed In open state- act as pores for selected ions (electrochemical gradient) After opening, channels return to closed state as a function of time Drugs termed potentiators (e.g., ivacaftor) may increase probability that a channel is in open state 5
- 6. Transporters Versus Channels Transporters Transporter- forms intermediate complex with substrate (solute) Subsequent conformational change in transporter Induces translocation of substrate to other side of membrane 6
- 7. Transporters Versus Channels Kinetics of solute movement differ between transporters and channels Particular transporter forms intermediate complexes with specific compounds (Substrates) 7
- 8. Mechanisms of Transport 8 Passive Diffusion Carrier mediated Transport Vesicular Transport Pore (Convective) Transport Ion Pair Formation • Facilitated Diffusion • Active Transport • Primary • Secondary • Carrier mediated intestinal Transport • Pinocytosis • Phagocytosis 1 2 3 4 5
- 9. 1. Passive Diffusion Nonionic diffusion (90% drugs) Molecules spontaneously diffuse from a region of higher concentration to a lower concentration Driving force- Solute’s Concentration (Electrochemical) gradient No external energy is required 9 Rate of Transfer= Flux
- 10. Passive Diffusion Best Expressed by- Fick’s law of diffusion (Adolf Fick) According to law- Drug molecules diffuse from a region of high drug concentration to a region of low drug concentration 10 dQ dt = DAK h (CGI - Cp) Surface area (A) Diffusion rate Thickness(h) Diffusion rate
- 11. Relationship between Molecular weight and Diffusion 11 Molecular Weight Diffusion
- 12. 2. Carrier mediated Transport Cell membranes possess specialised transport mechanisms Regulate entry and exit of physiologically important molecules Sugars, amino acids, neurotransmitters and metal ions Lipid soluble + Low molecular weight compound readily crosses membrane Suggest- presence of specialized transport mechanism Component of membrane called as Carrier 12
- 13. Carrier mediated Transport- Mechanism 13 • Carrier binds reversibly with solute molecule • Made complex • Travel across membrane to other side • Dissociated and discharge drug • Carrier return to its original site
- 14. CMT- Facilitated Diffusion Facilitated diffusion is a form of transporter-mediated membrane transport Does not require energy (Just as in passive diffusion) Saturable and structurally selective for drugs Shows competition kinetics for drugs of similar structure So, minor role in drug absorption 14
- 15. CMT- Facilitated Diffusion 15 • Both result in a final equilibrium distribution of a solute across membrane • Facilitated diffusion employs a specific transporter and exhibits Michaelise Menten saturation kinetics
- 16. Active Transport 16 Drug transported from a region of lower to one of higher concentration Against concentration gradient Uphill transport (Energy is required) Can be inhibited by metabolic poisoning that interfere with energy production (e.g, Fluoride, cyanide and dinitrophenol) 5-fluorouracil (Lipid insoluble drug)- Absorbed by GI
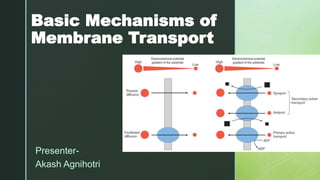
- 17. Active transport Depending on the driving force, divided into 2 types Primary active transport Secondary active transport Symport Antiport 17
- 18. Primary Active Transport Direct active transport or uniport ATP hydrolysis is coupled directly to solute transport 18 Low conc. High conc. It involves using energy (usually ATP) to directly pump a solute across a membrane against its electrochemical gradient.
- 20. P type- Na+ K+-ATPase Most important active transport protein This single enzyme accounts for one-third of human energy expenditure and is often referred to as the “pacemaker for metabolism.” Enzyme discovered in 1957 by Jens Skou (Nobel prize in chemistry, 1997) Na+ K+-ATPase is inhibited by digoxin, a cardiac glycoside 20
- 21. Secondary Active transport Also known as cotransport Transport across a biological membrane of solute against its concentration gradient is energetically driven by transport of another solute in accordance with its electrochemical gradient 2 types depending on transport direction of solute- Symporters or Antiporters 21
- 22. Secondary Active transport Ion gradient is coupled to movement of a solute in either: Same direction (symport) Opposite direction (antiport) Purpose of both types of co- transport is to use energy in an electrochemical gradient to drive the movement of another solute against its gradient 22
- 23. Secondary Active transport- Symport Example SGLT1 (sodium-glucose transport protein- 1) in intestinal epithelium Transport S2 and S1 in the same direction, as for glucose transport into the body from the lumen of the small intestine by the Na+-glucose transporter SGLT1 23
- 24. Secondary Active transport- Antiport Example Transporter moves S2 and S1 in opposite directions Using inwardly directed Na+ concentration gradient across the plasma membrane that the Na+,K+-ATPase maintains, the inward movement of 3 Na+ can drive the outward movement of 1 Ca++ via the Na+/Ca++ exchanger 24
- 25. Intestinal Transporters with e.g 25
- 26. 3. Vesicular Transport Process of engulfing particles or dissolved materials by cells to form a saccule or vesicle (This vesicles also called corpuscular or vesicular transport) 2 Process involved- 26 Cells excrete waste and other large molecules Vesicular Transported of solute
- 27. Vesicular Transport- Exocytosis Example Transport of protein such as insulin Insulin molecules are first packaged into intracellular vesicles then fuse with plasma membrane to release insulin outside the cell 27
- 28. Vesicular transport- Endocytosis 2 Types of endocytosis- Phagocytosis Pinocytosis 28 Fig- Cells excrete waste and other large molecules
- 29. Endocytosis- Phagocytosis Cell eating Uptake of large solid particles, often >0.5 mm Has surface proteins that specifically recognize and bind to the solid particles Phagocytosis is a routine process that ameba and ciliated protozoa use to obtain food 29
- 30. Endocytosis- Pinocytosis Cell drinking In humans, this process occurs in cells lining the small intestine and is used primarily for absorption of fat droplets 30
- 31. 4. Pore (Convective) Transport Very small molecules (Urea, water & sugars) are able to cross cell membrane rapidly if membrane contained channels or pores A certain type of protein called a transport protein may form an open channel across the lipid membrane of cell 31
- 32. 5. Ion Pair Formation Absorption of drugs like Quaternary ammonium compounds and sulfonic acids (Highly ionized or charged particles) Propranolol forms ion complex with oleic acid Quinine with hexylsalicylate 32
- 33. Ion Pair Formation- types 2 basic types of ion pairing (ionophores) Channel former Mobile former 33
- 34. Summary 34
- 35. References Goodman LS. Goodman and Gilman's the pharmacological basis of therapeutics. New York: McGraw-Hill; 2018. Shargel L, Andrew BC, Wu-Pong S. Applied biopharmaceutics & pharmacokinetics. Stamford: Appleton & Lange; 2005. Stillwell W. Membrane transport. An Introduction to Biological Membranes. 2013:305. https://dx.doi.org/10.1016%2FB978-0-444- 52153-8.00014-3. Flower RJ, Henderson G, Loke YK, MacEwan D, Rang HP. Rang & Dale's Pharmacology E-Book. Elsevier Health Sciences; 2018 Nov 4. Brahmankar DM, Jaiswal SB. Biopharmaceutics and pharmacokinetics: A treatise. Vallabh prakashan; 2005. 35
- 36. Thank you 36