Downloaded 88 times
![“There is now overwhelming evidence
that children with [specific] learning
disabilities do not have “holes in the
brain”. No ..studies have found a one-
to-one correlation between behavioural
symptoms and MRI or postmortem
pathology in [specific] learning
disabilities”C. Leonard, 1997, p 161
Because of UK/US differences in terminology, [specific] added for clarification
Leonard, C. M. (1997). Language and the prefrontal cortex. In N. Krasnegor, G. R. Lyon
& P. S. Goldman-Rakic (Eds.), Prefrontal cortex: Evolution, development, and behavioral
neuroscience (pp. 141-166). Baltimore: Paul H. Brookes.](https://image.slidesharecdn.com/sliandbrain-130204105553-phpapp02/75/SLI-and-the-brain-8-2048.jpg)

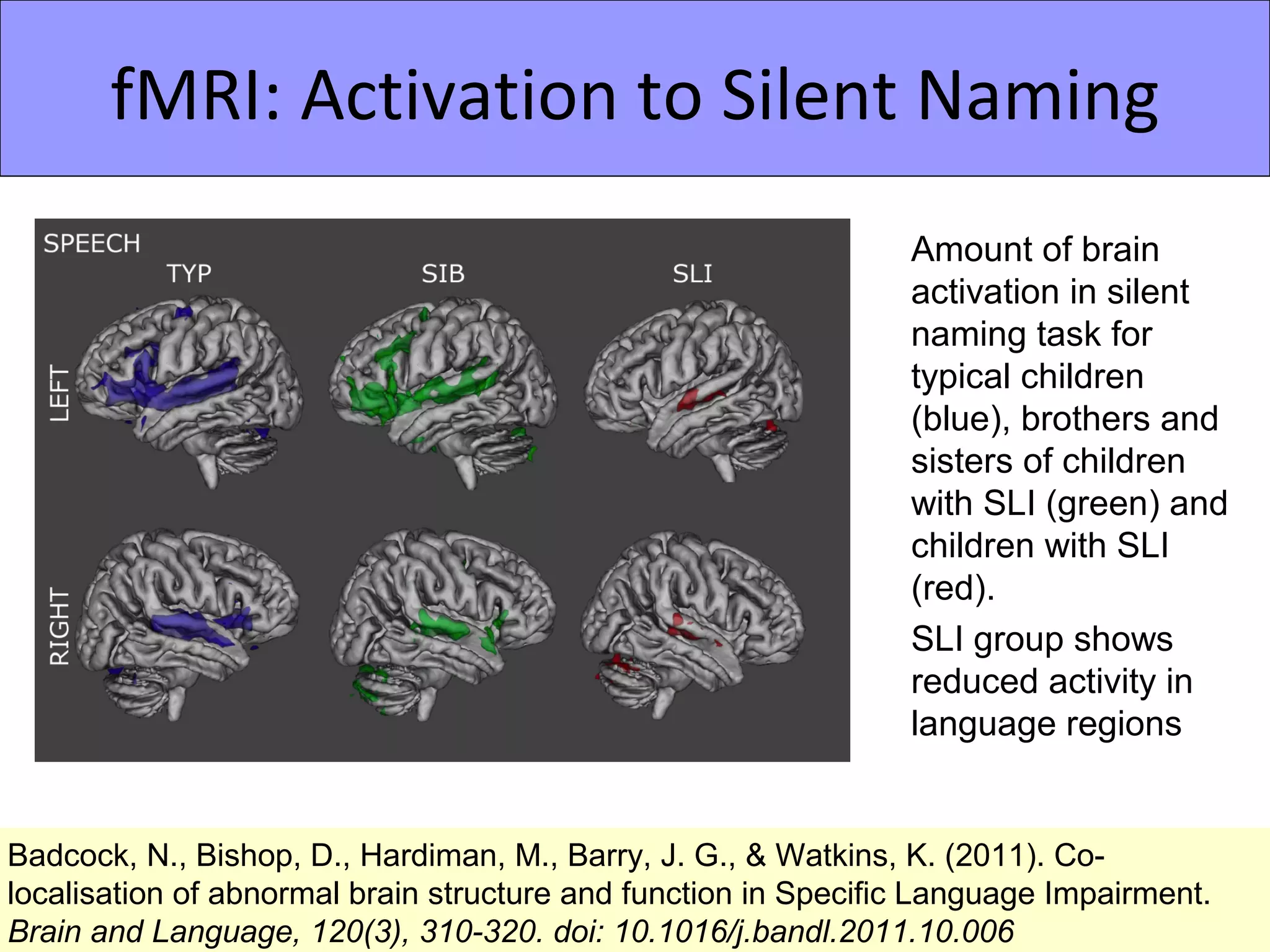
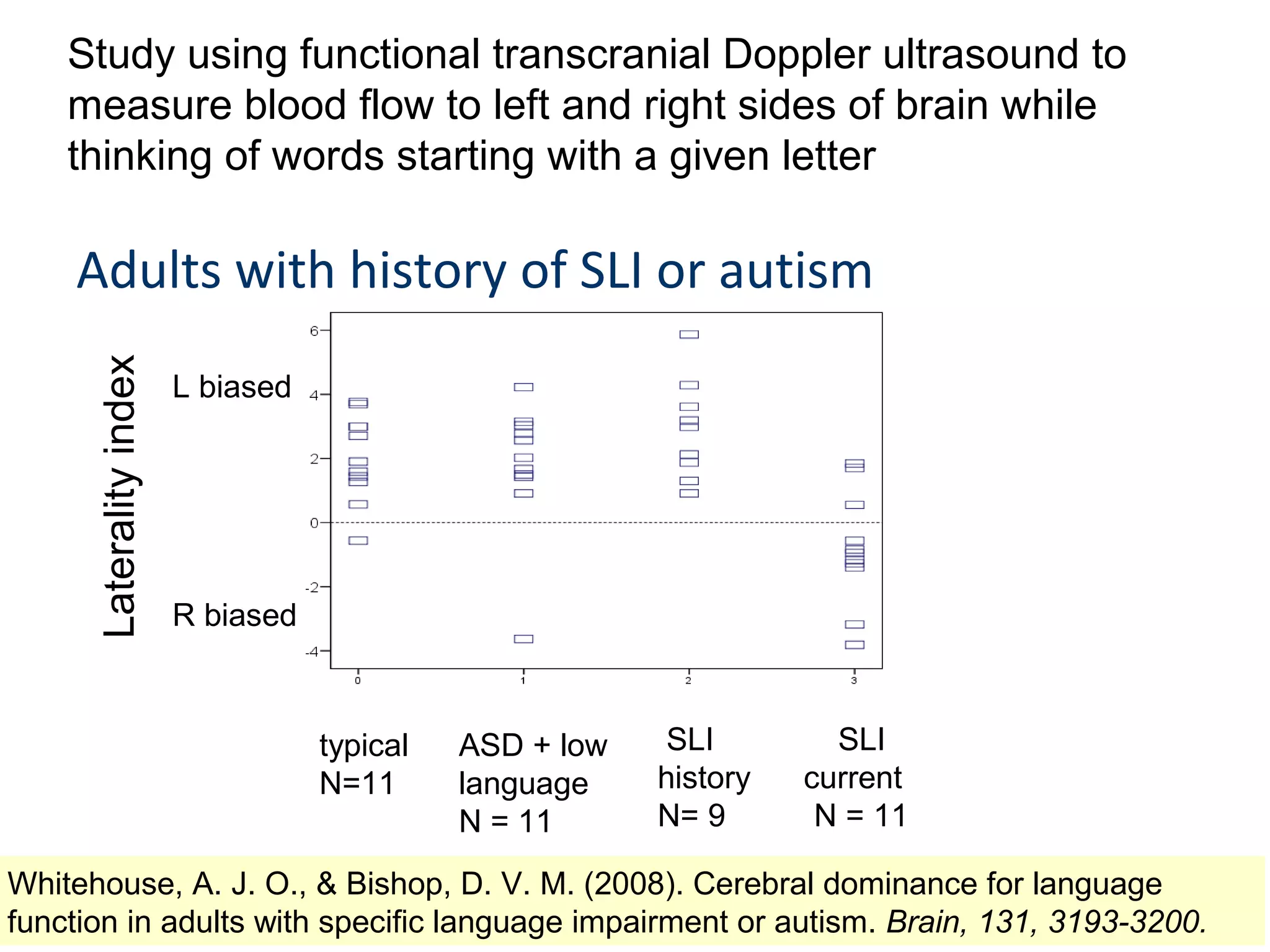
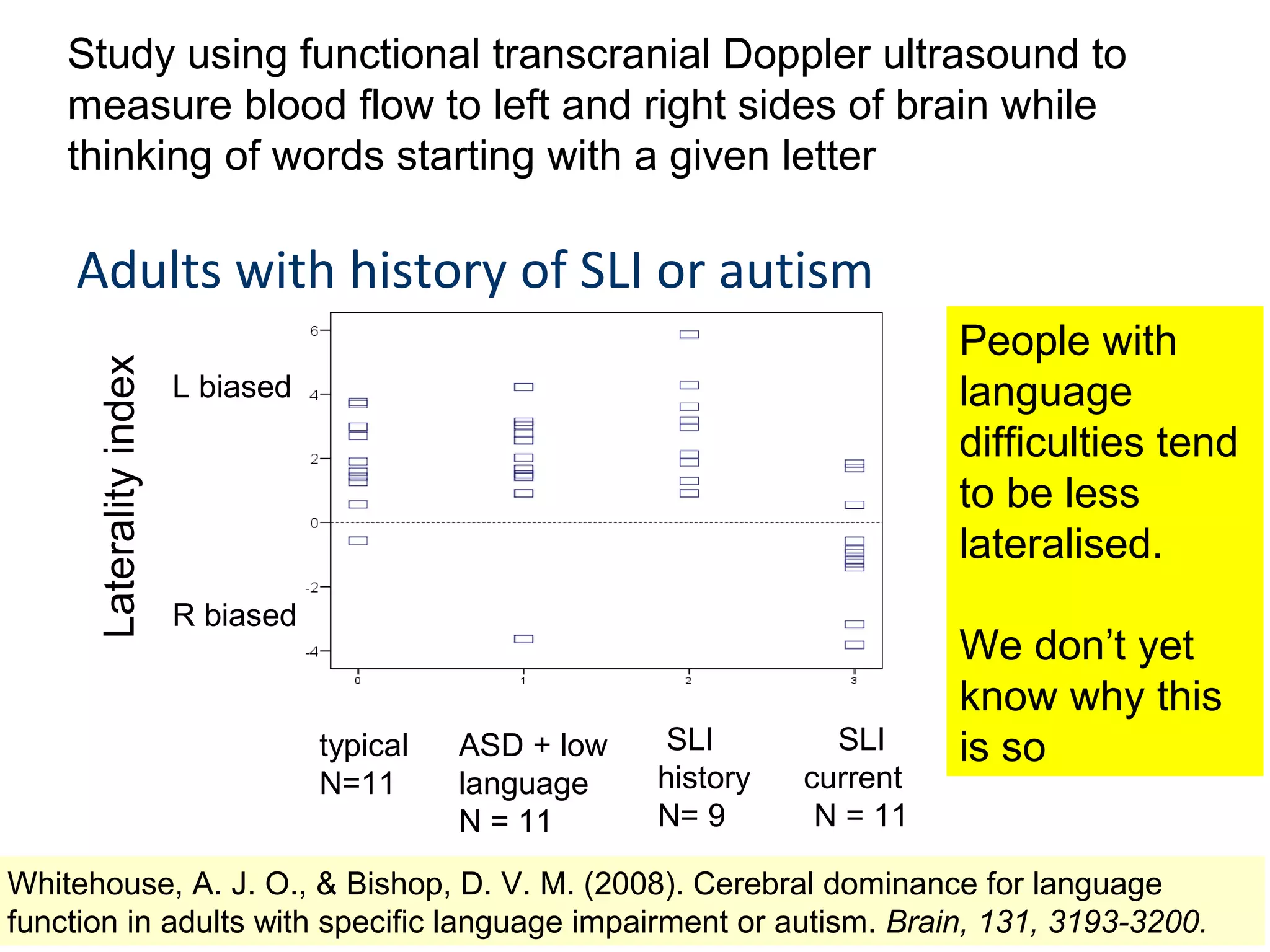


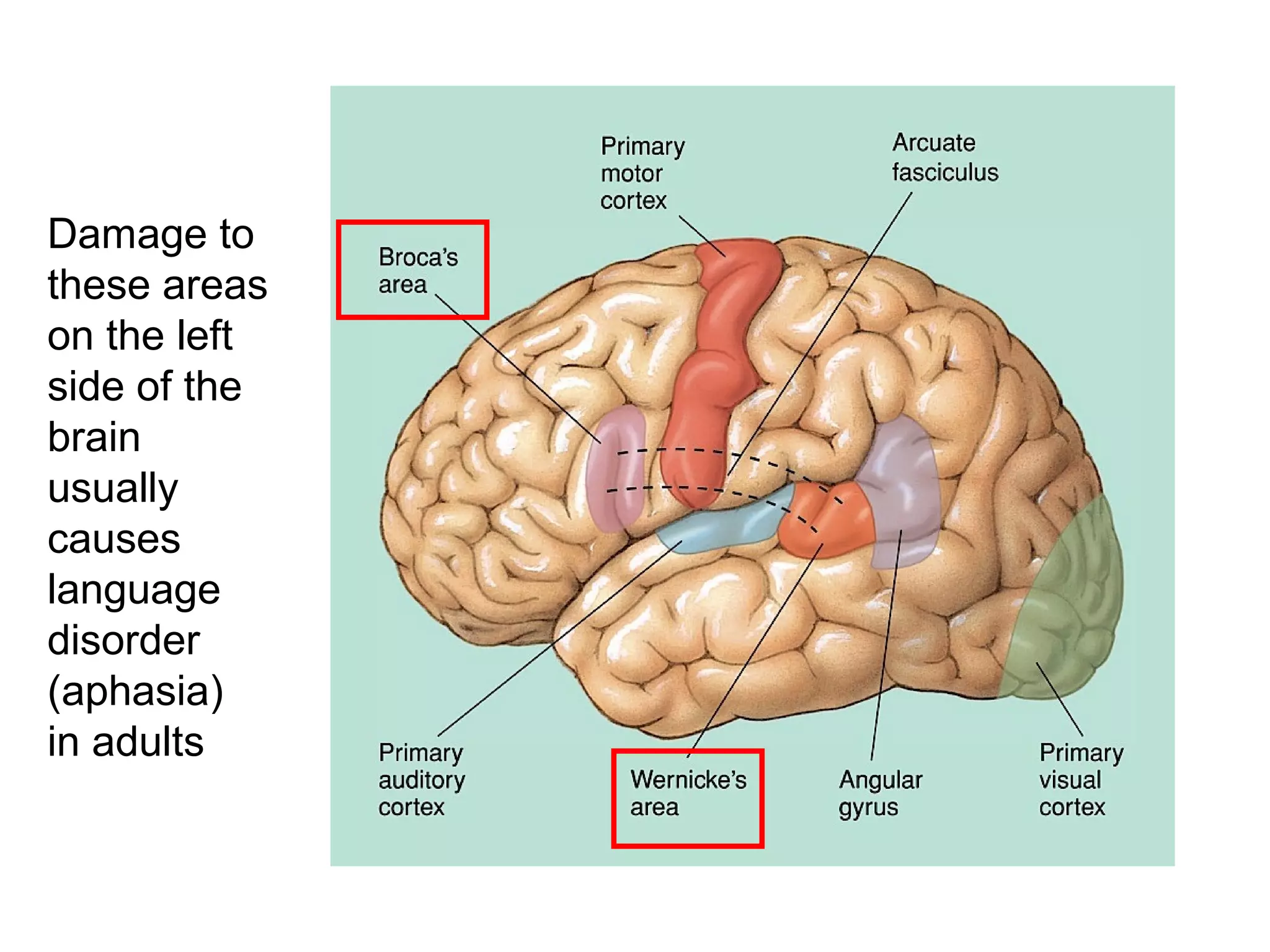
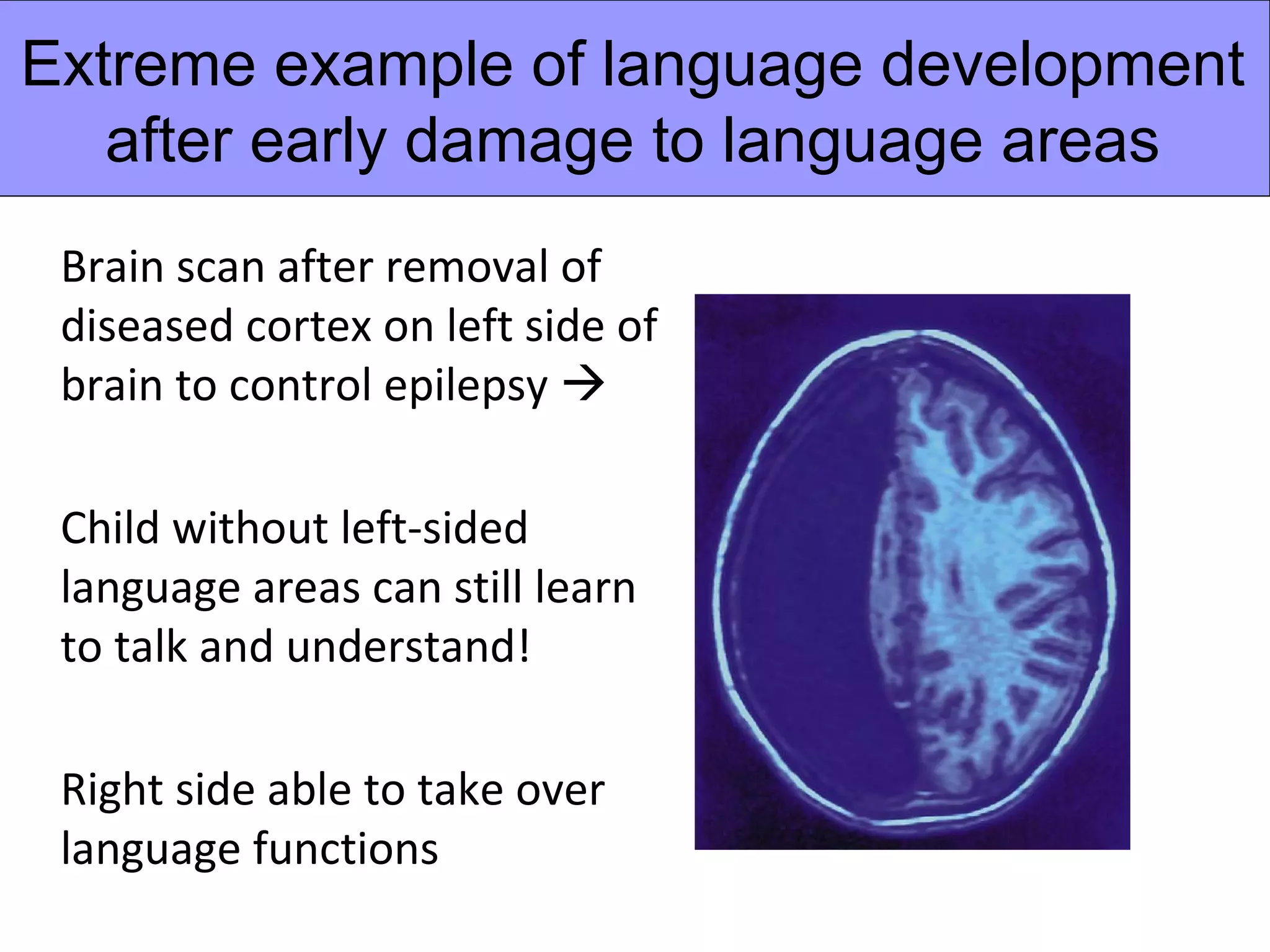
1) Specific language impairment (SLI) is not caused by brain damage like aphasia in adults, as brain scans do not typically show injuries in children with SLI unless they have other neurological issues. 2) Some studies have found subtle abnormalities in brain structure and function associated with SLI, such as minor differences in grey matter volumes or reduced activity in language areas during tasks. 3) People with a history of SLI may show weaker lateralization of language functions to the left side of the brain compared to typically developing individuals. However, the evidence from brain studies is mixed and abnormalities are often subtle or not present in all individuals with SLI.