
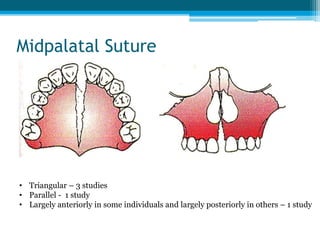
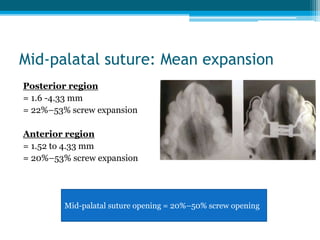
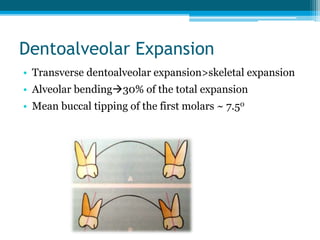
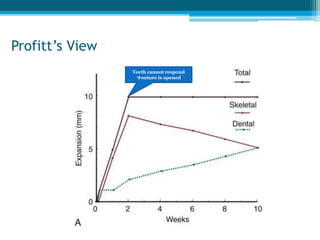
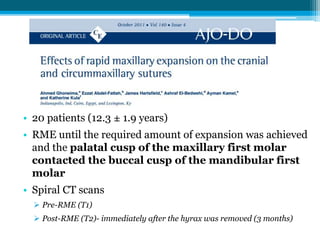
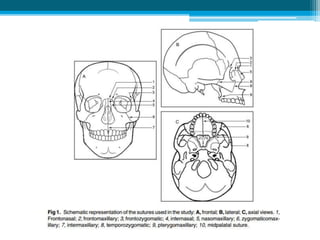
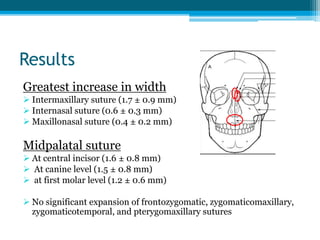
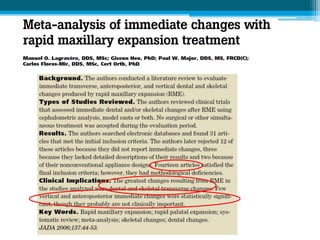
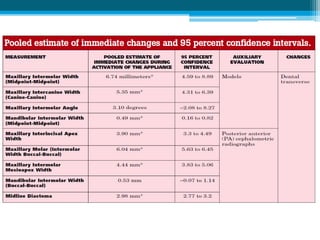
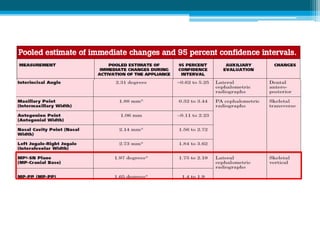
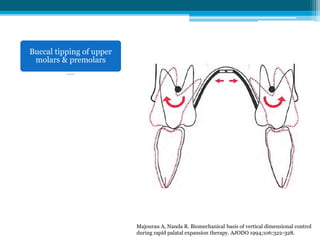
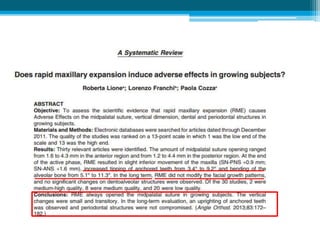

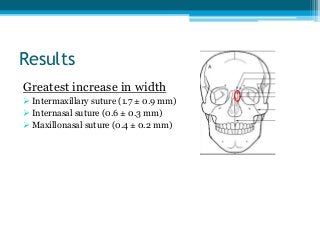
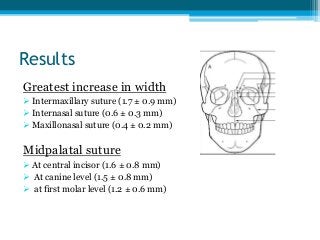
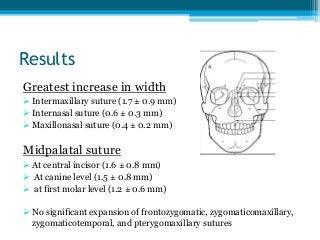
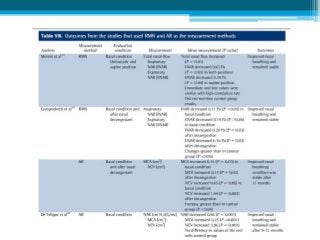
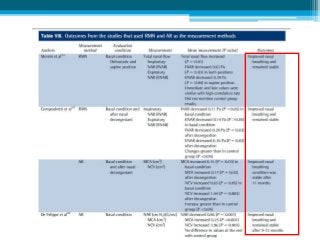

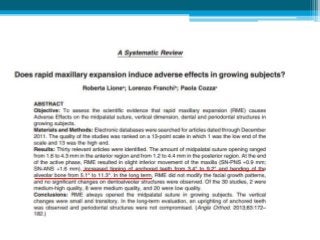


The document provides an overview of rapid maxillary expansion (RME), detailing its history, indications, types of appliances, and its effects on bone and airway. It highlights that RME primarily affects anterior sutures more than posterior ones and can improve nasal breathing, though vertical changes are minimal and temporary. Key findings include significant dentoalveolar expansion and the varying responses of cranial sutures to orthopedic forces.






![FACEMASK CHINCUP SEMINAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/facemaskchincupseminar1-230916061625-e0964de8-thumbnail.jpg?width=640&height=640&fit=bounds)




































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
















