
Recommended
Recommended
More Related Content
Similar to Financial Management Please respond to the following· Explain.docx
Similar to Financial Management Please respond to the following· Explain.docx (20)
More from voversbyobersby
More from voversbyobersby (20)
Recently uploaded
Recently uploaded (20)
Financial Management Please respond to the following· Explain.docx
- 1. "Financial Management" Please respond to the following: · Explain the three methods for calculating credit card interest and your reason for going with a particular method. · Provide an example of how you can use the power of compounding interest to pay for a future expense. · Discuss which practical application covered in the chapter you think you will use within the next year and how you think studying this topic will help you make wise financial choices in the future. ICU Nurses' Oral-Care Practices and the Current Best Evidence Author: Ganz, Freda DeKeyser, RN, PhD; Fink, Naomi Farkash, RN, MHA; Raanan, Ofra, RN, MA; Asher, Miriam, RN, BA; Bruttin, Madeline, RN, MA; Nun, Maureen Ben, RN, BSN; Benbinishty, Julie, RN, BA ProQuest document link Abstract: The purpose of this study was to describe the oral-care practices of ICU nurses, to compare those practices with current evidence-based practice, and to determine if the use of evidence-based practice was associated with personal demographic or professional characteristics. A national survey of oral-care practices of ICU nurses was conducted using a convenience sample of 218 practicing ICU nurses in 2004-05. The survey instrument included questions about demographic and professional characteristics and a checklist of oral-care practices. Nurses rated their perceived level of priority concerning oral care on a scale from 0 to 100. A score was computed representing the sum of 14 items related to equipment, solutions, assessments, and techniques associated with the current best evidence. This score was then statistically analyzed using ANOVA to determine differences of EBP based on demographic and professional characteristics.
- 2. The most commonly used equipment was gauze pads (84%), followed by tongue depressors (55%), and toothbrushes (34%). Chlorhexidine was the most common solution used (75%). Less than half (44%) reported brushing their patients' teeth. The majority performed an oral assessment before beginning oral care (71%); however, none could describe what assessment tool was used. Only 57% of nurses reported documenting their oral care. Nurses rated oral care of intubated patients with a priority of 67+/-27.1. Wide variations were noted within and between units in terms of which techniques, equipment, and solutions were used. No significant relationships were found between the use of an evidence-based protocol and demographic and professional characteristics or with the priority given to oral care. While nurses ranked oral care a high priority, many did not implement the latest evidence into their current practice. The level of research utilization was not related to personal or professional characteristics. Therefore attempts should be made to encourage all ICU nurses to introduce and use evidence- based, oral-care protocols. Practicing ICU nurses in this survey were often not adhering to the latest evidence-based practice and therefore need to be educated and encouraged to do so in order to improve patient care. Links:Check for Full Text Full text: Headnote Abstract Purpose: The purpose of this study was to describe the oral-care practices of ICU nurses, to compare those practices with current evidence-based practice, and to determine if the use of evidence-based practice was associated with personal demographic or professional characteristics. Design: A national survey of oral-care practices of ICU nurses was conducted using a convenience sample of 218 practicing ICU nurses in 2004-05. The survey instrument included
- 3. questions about demographic and professional characteristics and a checklist of oral-care practices. Nurses rated their perceived level of priority concerning oral care on a scale from 0 to 100. A score was computed representing the sum of 14 items related to equipment, solutions, assessments, and techniques associated with the current best evidence. This score was then statistically analyzed using ANOVA to determine differences of EBP based on demographic and professional characteristics. Findings: The most commonly used equipment was gauze pads (84%), followed by tongue depressors (55%), and toothbrushes (34%). Chlorhexidine was the most common solution used (75%). Less than half (44%) reported brushing their patients' teeth. The majority performed an oral assessment before beginning oral care (71%); however, none could describe what assessment tool was used. Only 57% of nurses reported documenting their oral care. Nurses rated oral care of intubated patients with a priority of 67±27.1. Wide variations were noted within and between units in terms of which techniques, equipment, and solutions were used. No significant relationships were found between the use of an evidence-based protocol and demographic and professional characteristics or with the priority given to oral care. Conclusions: While nurses ranked oral care a high priority, many did not implement the latest evidence into their current practice. The level of research utilization was not related to personal or professional characteristics. Therefore attempts should be made to encourage all ICU nurses to introduce and use evidence-based, oral-care protocols. Clinical Relevance: Practicing ICU nurses in this survey were often not adhering to the latest evidence-based practice and therefore need to be educated and encouraged to do so in order to improve patient care. Key words Oral care, intubated patient, evidence-based nursing practice Some members of the Israeli Cardiology and Critical Care
- 4. Nursing Society took the initiative to organize a work group dedicated to promoting critical care nursing research and evidence-based practice. The group first heard lectures about evidence-based practice and how it can clinically affect patient care and how to critically review the literature. Following these lectures, the group conducted lengthy discussions about the purpose of the group and what projects could be realistically completed. Members of the group came to the conclusion that they wanted to conduct a national project related to a clinical area that is exclusive to nursing, could apply to all types of intensive care units, had some evidence in the literature, and could affect patient outcomes. At the time of the beginning of the project (late 2003 to early 2004), several studies were published that found that poor oral hygiene might be associated with an increased risk for pneumonia with its concomitant increased morbidity and mortality. One specific article caught the attention of the group (Grap, Munro, Ashitani, & Bryant, 2003). These authors reported that intensive care unit (ICU) nurses' oral care practices were not documented nor were they in accordance with the most recent evidence. Oral care of intubated patients was then chosen as the topic for the project. Members of the group also believed that no consistent practices related to oral care existed, even within the same unit, and that most nurses had little or no knowledge of the current best evidence-based practice. Because the primary purpose of the group was to promote evidence-based practice, members were interested in determining what factors could be associated with the use of evidence in practice so that future interventions could be directed toward those groups to improve clinical practice and patient care. Therefore the purpose of the project was three fold: (a) to describe oral-care practices of ICU nurses, (b) to compare those practices to the current evidence, and (c) to determine whether personal demographic or professional characteristics were related to evidence-based, oral-care practice.
- 5. Background Ventilator-associated pneumonia (VAP) is considered to be the most common nosocomial infection (Vincent, 2004) and has been found to be a major cause of morbidity and mortality in ICUs (Bercault & Boulain, 2001; Elward, Warren, & Fraser, 2002; Relio et al., 2002). In a review of VAP literature, Chastre and Fagon (2002) concluded that VAP is a complication in 8%- 28% of patients receiving mechanical ventilation and causes a high mortality rate of 24%-50%. Several reports of studies have been published that indicated that oral decontamination might be associated with decreased risk for VAP (Bergmanns et al., 2001; Hubmayr, 2002; van Nieuwenhoven et al., 2004). Therefore, nurses could directly affect the level of VAP by providing effective oral care to decrease this contamination. Some investigators have shown that nurses based their oral-care practices on tradition, used many different techniques and products for oral care, and had no uniform method of oral assessment (Binkley, Furr, Carrico, & McCurren, 2004; Bowsher, Boyle, & Griffiths, 1999; Curzio & McCowan, 2000; Evans, 2001; Furr, Binkley, McCurren & Carrico, 2004; Grap et al., 2003; Jones, Newton & Bower, 2004; McNeill, 2000; Munro & Grap, 2004; Munro & Grap, 2004; Stiefel, Damron, Sowers & Velez, 2000; White, 2000). Grap et al. (2003) concluded that ICU nurses' oral-care practices were not documented nor were they in accordance with the most recent evidence. Similar results were found in several later studies conducted in the United States (Binkley et al., 2004; Cutler & Davis, 2005; Hanneman & Gusick, 2005) and in a survey of 59 European ICU nurses (Relio et al., 2007); but not by Jones et al. (2004) who found that UK nurses did perform appropriate oral care methods. When our evidence-based nurse (EBN) group was trying to decide which protocol to recommend, we found no consensus in the literature about what was the best evidence related to oral care. In a recent systematic review, Berry, Davidson, Masters,
- 6. & Rolls (2007) concluded that scarce evidence exists related to oral care practices of intubated ICU patients. The Centers for Disease Control and Prevention (CDC) staff have developed guidelines for preventing VAP (R). These guidelines include hand washing; education of healthcare workers about nosocomial pneumonia and its prevention; wearing of gloves; sub-glottic suctioning; head of bed elevation; and use of Chlorhexidine for cardiac-surgery patients. The last element of the CDC guideline for preventing VAP is the development of a comprehensive oralhygiene program; however, details are lacking about what the program should include. Another relevant set of guidelines from the CDC and the American Association of Critical Care nurses is the "ventilator bundle," that includes steps to reduce the incidence of VAP for mechanically ventilated patients. This bundle includes elevating the head of the bed, continuous subglottal suctioning, changing ventilator circuit no more than every 48 hours, and hand washing before and after contact with each patient. This protocol does not even mention oral care (Tolentino-DelosReyes, Ruppert, Shyang-Yun, & Shiao, 2007). Therefore, even though, in principle, oral care is considered of great importance to intubated and ventilated patients, its place in many guidelines related to these patients is unclear. Many studies have been conducted in order to determine what barriers are associated with a lack of evidencebased practice (EBP). Most of these studies have used the Barriers questionnaire developed by Funk and colleagues (1991), which groups these barriers into four basic categories: qualities of the research; presentation and accessibility of the research; setting or organizational barriers and limitations; and nurses' research values, skills, and awareness. Few researchers have investigated whether individual characteristics of nurses may be related to such perceptions. In many other countries around the world, there is access to nursing research (for example access to the Internet), but the culture of nursing research is not well developed. Ricart and
- 7. colleagues (2003) comment that variability in following evidence-based guidelines may be because of differences in training or cultural aspects of the country. In a recent article, Rassin (2008) found that nursing research was rated last in a list of 20 professional values among Israeli hospital nurses. This result is not surprising given the fact that nursing research capacity and exposure is relatively low in Israel (Ehrenfeld, Itzhaki, & Baumann, 2007; Glazer & DeKeyser, 2000). Most research is conducted by nurses obtaining an advanced degree and no national mechanisms are in place for designated funding for nursing research or for promoting EBP. Because no information was available about the current state of evidence-based oral care practice in Israel, the group decided to conduct a survey describing current oral-care practices of ICU nurses with intubated patients and to determine whether evidence-based practices were related to personal demographic or professional characteristics. Methods Sample A convenience sample of 218 practicing ICU nurses was obtained in 2004-2005. Members of the EBN group recruited nurses from their own ICUs, with some also recruiting nurses from other units within the same organization. Nurses in the survey worked in 12 different ICUs, 5 in general-respiratory ICUs, 3 in cardiovascular-surgical ICUs, 2 in neurosurgical ICUs and 2 in cardiac care ICUs. Instrument The survey included two major sections. The first section contained questions about demographic and professional characteristics including age, gender, nursing education, years of ICU experience, postbasic ICU certification, type of ICU, work full or part time, and shifts worked. The second section contained a checklist which included a listing of the current oral-care practices including type of equipment used, solutions used, technique, and the type and timing of oral assessment. Nurses were asked to check off all
- 8. responses that applied to their practice. Some of the items on the checklist were based on current best evidence, for example the use of Chlorhexidine or toothpaste; however, other items listed were not recommended, such as bicarbonate or lemon water. Nurses were also asked their perceived level of priority of oral care on a scale from 0 to 100. This question had a visual analogue format in which descriptors were placed at each end (highest priority= 100; lowest priority=0) on a 10-cm line. Nurses were asked to mark an X on the place that corresponded with the level of priority they gave to oral care. The survey instrument was based on the literature and constructed by a committee of experienced ICU nurses. Content validity of the tool was improved by including questions suggested by members of the EBN task force and consultants. The survey was also sent for review to an instructor of dental hygiene and to other ICU nurses for obtaining content validity. Reviewers were asked to suggest additional items or remove those which were listed. The final survey questionnaire was a conglomeration of the items suggested by the EBP group and those of the reviewers. The use of Cronbach's alpha for this tool was not deemed appropriate because the questionnaire is a checklist. Data Collection Each member of the EBN group obtained both ethical and institutional approval to collect the data. Then group members explained the study to nurses in a staff meeting, obtained informed consent from participants, and distributed the questionnaires on an individual basis. Nurses were asked to return the questionnaires to an envelope placed in a convenient location on each unit. Data Analysis Descriptive statistics, including measures of central tendency and dispersion and frequency data were used to describe the sample as well as responses to the oralcare practices survey. Not all participants completed all of the items - and these were not included in missing-data analyses.
- 9. An EBP score was also determined, which was defined as the number of items on the checklist that were checked off by the nurse and considered to be necessary for proper oral care according to the literature. Supplies listed included a toothbrush, suction and suction catheter, toothpaste, Chlorhexidine, and petroleum jelly (6 items). Technique items included care of the upper and lower mouth, tongue, and brushing of the patient's teeth (4 items). Assessment questions were about doing an assessment upon admission to the unit and at each shift (2 items). Use of an assessment tool and results of the assessment and oral care were to be charted accordingly (2 items) - for a total of 14 items. Each nurse obtained a score corresponding to the total number of evidence-based items checked off (from ?? 4). A higher score shows higher use of evidence-based practices. This total score was then correlated with demographic and professional characteristics to determine if such characteristics were associated with oral-care EBP. Data were collected on questionnaires that were delivered to one of the researchers, who then coded the data into an SPSS data file (Version 12). This score was then analyzed to determine whether a difference in EBP scores existed based on personal demographic or professional characteristics using ANOVA. Interval level independent variables were categorized as follows: age (years): 20-29, 30-39, 40-49, 50+; years of clinical experience (as RN, as an ICU nurse, and in this particular ICU): 0-5, 6-9, 10-14, 15-20, 20+; percentage of time worked: <50%, 50-75%, 75- 99%, 100%). All other variables were categorical (gender, education, type of ICU). Results The majority of the sample was female (?= 172, 82%) with an average age of 37.4+8.6 years. Nurses were mostly registered nurses with a baccalaureate degree who had completed a postbasic certification course (see Table 1). According to the latest available statistics of the Nursing Division of the Israel Ministry of Health (Nursing Division, Ministry of Health,
- 10. 2007), 76% of nurses in Israel are registered nurses; 25% have a baccalaureate degree or higher; and 41% have completed some form of postbasic certification. One tenth of nurses were male and 39% of all nurses were age 30-44 years. Nurses in this sample were better educated than the general population of Israeli nurses but otherwise seemed to be similar. The most commonly used supplies were gauze pads (n=182, 84%), followed by tongue depressors (n=118, 55%), and toothbrushes (n=73, 34%). Often nurses attach gauze pads to a tongue depressor to use for oral care - a practice that substitutes for the use of sponges or swabs attached to a stick sometimes done in other countries. Chlorhexidine was the most commonly used solution (n=161, 75%) followed by petroleum jelly (n=87, 40%), and toothpaste (n=72, 33%). Almost all nurses performed oral care (n=198, 91%); however, less than half (n=96, 44%) brushed their patients' teeth. Only 57% (n=120) of nurses reported documenting oral care. On a scale of 0-100, nurses rated oral care for intubated patients with a priority of 67+27.1, where 44% (n=96) rated it on a priority of 90%-100%. The mean EBP score was 9/14 or 68%. All participants stated that no known written oral-care protocol existed on their unit (see Table 2). No significant relationship was found between the use of evidence-based practices and demographic or professional characteristics or with the priority given to oral care. Discussion While nurses ranked oral care as a high priority, many did not implement the latest evidence into their current practice. The level of evidence-based practice was not related to personal demographic or professional factors. Perceived level of priority of oral care practices has been measured differently in different studies but for the most part many studies have shown that critical care nurses rate oral care with a moderate to high priority, including the nurses in this study (Binkley et al., 2004; Grap et al., 2003; Jones et al., 2004; Relio et al., 2007).
- 11. As in previous studies (Binkley et al., 2004; Grap et al., 2003; Relio et al., 2007; Ricart et al., 2003), the level of EBP has been questionable. Many nurses in this sample did not implement the latest evidence in their practice. The American Association of Critical Care Nurses produced a "practice alert" based on the current best evidence, describing recommended oral care in the critically ill (American Association of Critical Care Nurses [AACN], 2007). AACN recommendations included developing an oralcare hygiene program which includes brushing patients' teeth, gums, and tongue at least twice a day, using a soft pediatric or adult toothbrush, moisturizing oral mucosa and lips every 2-4 hours, and in precardiac surgery patients - using oral Chlorhexidine gluconate (0.12%) rinse twice a day. All of the nurses in our study stated that no organized protocols or programs related to oral hygiene existed on their units. Most did not brush their patients' teeth. It is not known what type of toothbrush was used among those that did brush their patients' teeth. However, almost all of the respondents (8491%) claimed to clean their patients' tongue and upper and lower mouth. Petroleum jelly, a substance used to moisturize the lips, was used by many of the respondents; however, the frequency of use was not reported. The majority of nurses on all of the units reported using Chlorhexidine, a substance that has received scientific support for use in a very limited population-precardiac surgery patients. This solution was not recommended for other patient populations. A wide range of practices was found in this study among nurses working within the same unit and between units, partially because of the fact that no known written oral-care protocols existed. Several authors have commented on the importance of using written protocols in guiding oral care (Cason, Tyner, Saunders, & Broome, 2007; Cutler & Davis, 2005; Steifel et al., 2000). None of the individual nurse characteristics in this study were found to be related to evidence-based practice or priority of oral
- 12. care. The only characteristics found in the literature to be related to evidence-based practice were educational level, nursing position, and experience. Several investigators have found that the higher the level of academic nursing education, the more positive the attitude toward nursing research and EBP (Bonner & Sando, 2008; Bucknall, Copnell, Shannon, & McKinley, 2001; Fink, Thompson, & Bonnes, 2005; Furr et al., 2004; Hannes et al., 2007; Kajermo et al., 2008); however, Oh (2008) and Roxburg (2006) found the opposite results. In a recent study of Israeli hospital nurse values (Rassin, 2008), the findings were that nurses with a baccalaureate degree valued nursing research more than any other type of nurse, including those with a master's degree. The authors did not explain this result but the finding is in keeping with a discrepancy in the literature. The literature is also ambiguous regarding the influence of nursing position on attitudes toward research and EBP. While several authors (Bonner & Sando, 2008; Egerod & Hansen, 2005; Oh, 2008) found that higher level positions were associated with more positive attitudes, Bucknall et al. (2001) found the opposite result. Oh (2008) determined that level of nursing experience was associated with more positive attitudes, while Furr et al. (2004) found the opposite. In these studies, the researchers defined attitudes toward EBP differently and the studies were conducted using different designs and in different cultures therefore conflicting findings are not too surprising. However, many of the studies using the barrier scale found that one of the greatest barriers to evidence-based practice was the nurses' assessment of her lack of skills related to use of research. Perhaps increased education, experience, and a higher position may be related to increased feelings of competence related to research. Based on the results of this study, where no oral care protocols were reported and where there were no differences between nurses based on personal or professional characteristics related to the use of EBP, it is recommended that standardized, written,
- 13. evidence-based protocols related to the oral assessment and care be introduced into all ICUs admitting intubated patients. Nurses at all levels should be informed and encouraged in its use. Further research could include investigating other barriers related to EBP in this area and in this culture, as well as what other factors are associated with the introduction and use of evidence-based protocols. Conclusions While nurses ranked oral care as a high priority, levels of EBP were found to be relatively low. Demographic and professional characteristics were not found to be associated with the use of EBP. Therefore, all nurses, regardless of personal characteristics, should be involved in educational programs related to oral care and evidence-based practice and should be encouraged to introduce and utilize written protocols based on the latest evidence in an attempt to decrease VAP on their units. Acknowledgements This study was supported by the Israeli Cardiology and Critical Care Nursing Society. Clinical Resource * Practice Alert of the American Association of Critical Care Nurses: http://www.aacn.org/WD/ practice/docs/oraLcare Jn _the.critically.ill.pdf References References American Association of Critical Care Nurses. (2207). Practice alert, oral care in the critically ill. Retrieved April 20, 2007, from http:www.aacn.org Bercault, N., & Boulain, T. (2001). Mortality rate attributable to ventilator associated nosocomial pneumonia in an adult intensive care unit: A prospective case control study. Critical Care Medicine, 29, 2303-2309. Bergmanns, D.C.J.J., Bonten, M.J. M., Gaillard, CA., Paling, J. C, van der Geest, S., van Teil, F. H., et al. (2001 ). Prevention of ventilator-associated pneumonia by oral decontamination. American Journal of Respiratory Care, 164, 382-388.
- 14. Berry, A.M., Davidson, P.M., Masters, J., & Rolls, K. (2007). Systematic literature review of oral hygiene practices for intensive care patients receiving mechanical ventilation. American Journal of Critical Care, 16, 552-563. Binkley, C, Furr, A, Carneo, R., & McCurren, C. (2004). Survey of oral care practices in U.S. intensive care units. American Journal of Infection Control, 32, 161-169. Bonner, A., & Sanso, J. (2008). Examining the knowledge, attitude and use of research by nurses. Journal of Nursing Management, 16, 334-343. Bowsher, J., Boyle, S., & Griffiths, J. (1999). Oral care. Nursing Standard, 13(37), 31. Bucknall, T., Copnell, B., Shannon, K., & McKinley, D. (2001). Evidence-based practice: Are critical care nurses ready for it? Australian Critical Care, 14, 92-98. Cason, CL., Tyner, T., Saunders, S., & Broome, L. (2007). Nurses' implementation of guidelines for ventilator-associated pneumonia from the Centers for Disease Control and Prevention. American Journal of Critical Care, 16, 28-36. Chastre, J., & Fagon, J.Y. (2002). Ventilator-associated pneumonia. American Journal of Respiratory and Critical Care Medicine, 165, 867-903. Curzio, J., & McCowan, M. (2000). Getting research into practice: Developing oral hygiene standards. British Journal of Nursing, 9, 434-438. Cutler, C.J., & Davis, N. (2005). Improving oral care in patients receiving mechanical ventilation. American Journal of Critical Care, 14, 389-394. Egerod, I., & Hansen, G. M. (2005). Evidence-based practice among Danish cardiac nurses: A national survey. Journal of Advanced Nursing, 51, 465-473. Ehrenfeld, M., Itzhaki, M., & Baumann, S. L. (2007). Nursing in Israel. Nursing Science Quarterly, 20, 372-375. Elward, A.M., Warren D.K., & Fraser V.J. (2002). Ventilator associated pneumonia in pediatric intensive care unit patients: Risk factors and outcomes. Pediatrics, 109, 758-764.
- 15. Evans, G. (2001). A rationale for oral care. Nursing Standard, 15(43), 33-36. Funk, S. G., Champagne, M.T., Wiese, RA., & Tornquist, E. M. (1991). Barriers: The barriers to research utilization scale. Applied Nursing Research, 4, 39-45. Fink, R., Thompson, CJ., & Bonnes, D. (2005). Overcoming barriers and promoting the use of research in practice. Journal of Nursing Administration, 35, 121-129. Furr, LA., Binkley, CJ., McCurren C, & Carrico, R. (2004). Factors affecting quality of oral care in intensive care units. Journal of Advanced Nursing, 48, 454-462. Glazer, G., & DeKeyser, F. (2000). Prerequisites and priorities for nursing research in Israel. Online Journal of Issues in Nursing, 5. Grap, M.J., Munro, CL., Ashtiani, B., & Bryant, S. (2003). Oral care interventions in critical care: Frequency and documentation. American Journal of Critical Care, 12, 113-119. Hanneman, S. K., & Gusick, G. M. (2005). Frequency of oral care and positioning of patients in critical care: A reflection. American Journal of Critical Care, 14, 378-387. Hannes, K., Vandersmissen, J., DeBlaeser, L., Peeters, G., Goedhuys, J., & Aertgeerts, B. (2007). Barriers to evidence- based nursing: A focus group study. Journal of Advanced Nursing, 60, 162-171. Hubmayr, R. D. (2002). Statement of the 4th international consensus conference in critical care on ICU-acquired pneumonia. Intensive Care Medicine, 28, 1521-1536. Jones, H., Newton, J.T., & Bower, E.J. (2004). A survey of oral care practices of intensive care nurses. Intensive and Critical Care Nursing, 20, 69-76. Kajermo, K. N., Unden, M., Gardulf, A. Erikssan, L.E., Orton, M., Arnetz, B. B. et al. (2008). Predictors of nurses' perceptions of barriers to research utilization. Journal of Nursing Management, 16, 305-314. McNeill, H. E. (2000). Biting back at poor oral hygiene. Intensive and Critical Care Nursing, 16, 367-372.
- 16. Munro, CL., & Grap, M.J. (2004). Oral health and care in the intensive care unit: State of the science. American Journal of Critical Care, 13, 25-34. Nursing Division, Israel Ministry of Health. (2007). Retrieved July 31, 2008, from http://www.moh.gov.il Oh, E.G. (2008). Research activities and perceptions of barriers to research utilization among critical care nurses in Korea. Intensive and Critical Care Nursing, 24, 314-322. Rassin, M. (2008). Nurses' professional and personal values. Nursing Ethics, 15, 614-630. Rello, J., Koulenti, D., Blot, S" Sierra, R" Diaz, E., De Waele, J.J. et al. (2007). Oral care practices in intensive care units: A survey of 59 European ICUs. Intensive Care Medicine, 33, 1066-1070. Relio, J., Ollendorf, DA., Oster, G., Vera-Llonch, M., Bellm, L., Redman, R. et al. (2002). Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest, 122, 2115-2121. Ricart, M., Lorente, C, Diaz, E., Kollef, M.H., & Relio, J. (2003). Nursing adherence with evidence-based guidelines for preventing ventilator-associated pneumonia. Critical Care Medicine, 31, 2693-2696. Roxburgh, M. (2006). An exploration of factors which constrain nurses from research participation. Journal of Clinical Nursing, 15, 535-545. Stiefel K.A., Damron, S., Sowers, N.J., & Velez, L. (2000). Improving oral hygiene for the seriously ill patient: Implementing research based practice. MedSurg Nursing, 9, 40- 46. Tablan, O. C, Anderson L.J., Besser, R., Bridges, C, & Hajjeh, R. (2004, March 26). Guidelines for preventing health-care associated pneumonia, 2003: Recommendations of CDC and the Healthcare Infection Control Practices Advisory Committee. Morbidity and Mortality Weekly Report, 53(RR-3), 1-36. Tolentino-DelosReyes, A. F., Ruppert, S.D., Shyang-Yun, & Shiao, P.K. (2007). Evidence-based practice: Use of the
- 17. ventilator bundle to prevent ventilator-associated pneumonia. American Journal of Critical Care, 16, 20-27. van Nieuwenhoven, CA., Buskens, E., Bergmans, D. C, van Tiel, F.H., Ramsay, G., & Bonten, M.J.M. (2004). Oral decontamination is cost-saving in the prevention of ventilator- associated pneumonia in intensive care units. Critical Care Medicine, 32, 126-130. Vincent, J. L. (2004). Ventilator-associated pneumonia. Journal of Hospital Infection, 57, 272-280. White, R. (2000). Nurse assessment of oral health: A review of practice and education. British Journal of Nursing, 9, 260-265. AuthorAffiliation Freda DeKeyser Ganz, RN1 PhD1, Naomi Farkash Fink, RN, MHA2, Ofra Raanan, RN, MA3, Miriam Asher, RN, BA4, Madeline Bruttin, RN, MA5, Maureen Ben Nun, RN, BSN6, & Julie Benbinishty, RN, BA7 1 Pi, Head, Master's Program, Hadassah-Hebrew University School of Nursing, Jerusalem, Israel 2 Nursing Research Coordinator, Rabin Medical Center, Petach Tikva, Israel 3 Instructor, Sheba-Tel Hashomer Medical Center, Tel Hashomer, Israel 4 Rabin Medical Center, Petach Tikva, Israel 5 Instructor, Recanati School of Health Professions, Ben Gurion University, Beer Sheva, Israel 6 Kaplan Medical Center, Rehovot, Israel 7 Instructor, Hadassah Hebrew University School of Nursing, Jerusalem, Israel AuthorAffiliation Correspondence DeKeyser Ganz, Hadassah-Hebrew University School of Nursing, Kiryat Hadassah, P.O. Box 12000, Jerusalem. E-mail: [email protected] Accepted: December 1 , 2008. dol: 10.1111/j.1547-5069.2009.01264.x
- 18. MeSH: Humans, Intensive Care Units -- statistics & numerical data (major), Nurses -- statistics & numerical data (major), Oral Hygiene (major), Physician's Practice Patterns -- organization & administration (major) Publication title: Journal of Nursing Scholarship Volume: 41 Issue: 2 Pages: 132-8 Number of pages: 7 Publication year: 2009 Publication date: Second Quarter 2009 Year: 2009 Section: CLINICAL SCHOLARSHIP Publisher: Blackwell Publishing Ltd. Place of publication: Indianapolis Country of publication: United Kingdom Publication subject: Education--Higher Education, Medical Sciences--Nurses And Nursing ISSN: 15276546 CODEN: IMNSEP Source type: Scholarly Journals Language of publication: English Document type: Journal Article Accession number: 19538697 ProQuest document ID: 236343430 Document URL: https://library.gcu.edu:2443/login?url=http://search.proqu est.com/docview/236343430?accountid=7374 Copyright: Copyright Blackwell Publishing Ltd. Second Quarter 2009 Last updated: 2014-06-28 Database: ProQuest Central Contact ProQuest Copyright © 2014 ProQuest LLC. All rights reserved. - Terms and Conditions
- 19. Journal of Evaluation in Clinical Practice, 12 , 3, 347–352 © 2006 Blackwell Publishing Ltd 347 Blackwell Science, LtdOxford, UKJEPJournal of Evaluation in Clinical Practice1356-1294Blackwell Publishing Ltd 200512 3347352 Original Article Grading strength of guideline recommendationsE. Roddy et al.
- 20. Correspondence Edward Roddy Academic Rheumatology Clinical Sciences Building Nottingham City Hospital Hucknall Road NG5 1PB UK E-mail: [email protected] Keywords: clinical guidelines, evidence-based medicine, strength of recommendation Accepted for publication: 27 April 2005 Evidence-based clinical guidelines: a new system to better determine true strength of recommendation Edward Roddy MRCP (Specialist Registrar in Rheumatology),
- 21. 1 Weiya Zhang PhD (Senior Lecturer in Musculoskeletal Epidemiology), 1 Michael Doherty MA MD FRCP (Professor of Rheumatology), 1 Nigel K. Arden MD MSc MRCP (Senior Lecturer in Rheumatology), 2 Julie Barlow PhD (Professor of Health Psychology), 3 Fraser Birrell MA PhD MRCP (Senior Lecturer in Rheumatology),
- 22. 4 Alison Carr PhD (Special Lecturer in Musculoskeletal Epidemiology), 1 Kuntal Chakravarty FRCP (Consultant Rheumatologist), 5 John Dickson FRCP MRCGP (Community Specialist in Rheumatology), 6 Elaine Hay MD FRCP (Professor of Community Rheumatology), 7 Gillian Hosie FRCP (General Practitioner), 8
- 23. Michael Hurley PhD (Reader in Physiotherapy & ARC Research Fellow), 9 Kelsey M. Jordan MRCP (Rheumatology Research Fellow), 2 Christopher McCarthy PhD (Research Physiotherapist), 10 Marion McMurdo MD FRCP (Professor of Ageing and Health), 11 Simon Mockett MPhil (Senior Lecturer), 12 Sheila O’Reilly MD MRCP (Consultant Rheumatologist),
- 24. 13 George Peat PhD MCSP (Research Fellow), 7 Adrian Pendleton MD MRCP (Specialist Registrar in Rheumatology), 14 Selwyn Richards MA MSc FRCP (Consultant Rheumatologist) 15 1 Academic Rheumatology, Clinical Sciences Building, Nottingham City Hospital, Hucknall Road, Nottingham, UK 2 MRC Epidemiology Resource Centre, Southampton General
- 25. Hospital, Tremona Road, Southampton, Hampshire, UK 3 Interdisciplinary Research Centre in Health, School of Health and Social Sciences, Coventry University, Priory St, Coventry, UK 4 Musculoskeletal Research Group, University of Newcastle upon Tyne, UK 5 Haroldwood Hospital, Gubbins Lane, Romford, Essex, UK 6 Langbaurgh PCT, Langbaurgh House, Bow Street, Guisborough, Cleveland, UK 7 Primary Care Sciences Research Centre, Keele University, Staffordshire, UK
- 26. 8 Primary Care Rheumatology Society, Northallerton, North Yorkshire, UK 9 King’s College London, Rehabilitation Research Unit, Dulwich Hospital, East Dulwich Grove, London, UK 10 The Centre for Rehabilitation Science, University of Manchester, Oxford Road, Manchester, UK 11 Department of Medicine, University of Dundee, Ninewells Hospital, Dundee, UK 12 Division of Physiotherapy Education, School of Community Health Sciences, University of Nottingham, Nottingham City Hospital, Hucknall Road, Nottingham, UK
- 27. 13 Derbyshire Royal Infirmary, London Road, Derby, UK 14 Craigavon Area Hospital, 68 Lurgan Road, Portadown, Co Armagh, UK 15 Poole Hospital, Longfleet Road, Poole, UK Abstract Rationale, aims and objectives Clinical practice guidelines often grade the ‘strength’ of their recommendations according to the robustness of the sup- porting research evidence. The existing methodology does not allow the strength of recommendation (SOR) to be upgraded for recommendations for which randomized controlled trials are impractical or unethical. The pur-
- 28. pose of this study was to develop a new method of determining SOR, incor- porating both research evidence and expert opinion. Methods A Delphi technique was employed to produce 10 recommendations for the role of exercise therapy in the management of osteoarthritis of the hip or knee. The SOR for each recommendation was determined by the traditional method, closely linked to the category of research evidence found on a systematic literature search, and on a visual analogue scale (VAS). Recommendations were grouped A-D according to the traditional SOR allocated and the mean VAS calculated. Difference across the groups was assessed by one- E. Roddy et al. 348
- 29. © 2006 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice , 12 , 3, 347–352 way ANOVA variance analysis. Results Mean VAS scores for the tradi- tional SOR groups A-D and one proposition which was ‘not recommended’ showed significant linearity on one-way
- 30. ANOVA . However, certain recom- mendations which, for practical reasons, could not assessed in randomized controlled trials and therefore could not be recommended strongly by the traditional methodology, were allocated a strong recommendation by VAS. Conclusions This new system of grading strength of SOR is less con- strained than the traditional methodology and offers the advantage of allowing SOR for procedures which cannot be assessed in RCTs for prac- tical or ethical reasons to be upgraded according to expert opinion. Introduction Clinical guidelines have been defined as ‘systemati- cally developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical conditions’ (Field & Lohr 1990). Guidelines that employ an evidence-based format currently grade each recommendation in two ways: first, by classifying the ‘category of evidence’ and, second, by giving a ‘strength of recommendation’. Although several methods of producing such grades
- 31. are described, in most of these, including the method most commonly used by clinical guidelines in rheu- matology (Pendleton et al . 2000; Jordan et al . 2003; Dougados et al . 2004; Zhang et al . 2004; Roddy et al . 2005), the latter is strongly dependent on the former (Shekelle
- 32. et al . 1999) (Table 1). That is, the strength of recommendation (SOR) primarily reflects the robustness of the research evidence, with evidence from randomized controlled trials (RCTs) and systematic reviews automatically conferring the strongest recommendation. However, although this traditional method allows a downgrading of the SOR for reasons including side effects or inconsistent studies, it does not allow an upgrading of recommen- dations in situations where RCTs are impractical or unethical, e.g. total joint replacement, but effective- ness is not in doubt. Furthermore, the practice of evidence-based medicine requires the integration of clinical expertise with the best available evidence from systematic research (Sackett et al . 1996). Dur- ing the development of recent recommendations for the role of exercise in the management of osteo- arthritis (OA) of the hip or knee (Roddy et al . 2005),
- 33. we found that the SOR allocated by this method was often discordant with the consensus opinion of the Table 1 Traditional hierarchy for category of evidence and strength of recommendation (Shekelle et al . 1999) Categories of evidence 1A. meta-analysis of RCT 1B. at least one RCT 2A. at least one CT without randomization 2B. at least one type of quasi-experimental study 3. descriptive studies (comparative, correlation, case-control) 4. expert committee reports/opinions and/or clinical opinion of respected authorities Strength of recommendation A. Directly based on category 1 evidence B. Directly based on category 2 evidence or extrapolated recommendation from category 1 evidence C. Directly based on category 3 evidence or extrapolated recommendation from category 1 or 2 evidence D. Directly based on category 4 evidence or extrapolated recommendation from category 1, 2 or 3 evidence
- 34. RCT, randomized controlled trial; CT, controlled trial. Grading strength of guideline recommendations © 2006 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice , 12 , 3, 347–352 349 panel. Therefore, we developed an alternative method to better capture the true opinion of the panel, whilst still requiring them to consider the research evidence. We examined whether this alter- native approach affected the support afforded to each recommendation.
- 35. Methods A multi-disciplinary panel employed a Delphi tech- nique to produce 10 recommendations relating to the role of exercise in the management of OA of the hip or knee (Roddy et al . 2005). Following a literature search and summary analysis of results, the evidence for each recommendation was assessed. The category of evidence and SOR was assigned for each according to the method previ- ously described (Shekelle et al . 1999). In addition, each participant was asked to indicate how strongly they rated each recommendation, based not just on research evidence but also on all aspects relating to their knowledge and clinical opinion. This was recorded using a 10-cm visual analogue scale (VAS) anchored with two descriptors labelled ‘not recom- mended at all’ at the far left (0 cm) and ‘fully rec- ommended’ at the far right (10 cm). The mean VAS and standard deviation for each recommendation were calculated. The recommendations were then
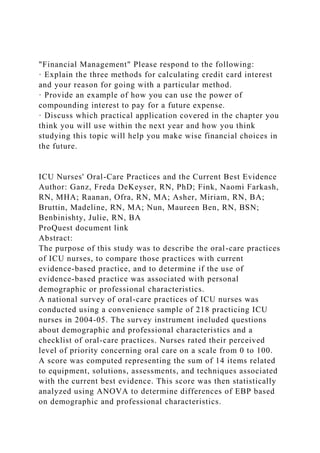
- 36. grouped according to their original SOR (A-D) and the mean VAS and 95% confidence interval calcu- lated for each group. A one-way ANOVA variance analysis was performed to assess the difference between the groups. Results The recommendations and the categories of evi- dence, SOR and VAS for each, are shown in Table 2. Figure 1 shows the mean VAS and 95% confidence interval for recommendation groups A, C and D in addition to one recommendation which was contra- dicted by the research evidence and could not there- fore be graded according to the traditional method (‘not recommended’). No recommendations were allocated a grade B SOR. The one-way ANOVA vari- ance analysis identified a significant difference across the groups ( P
- 37. < 0.001) and significant linearity ( P < 0.001). Discussion There was similarity between the SOR produced by this method and the traditional methodology (Shek- elle et al . 1999). The mean VAS for each recommen- dation group (A, C, D) increased with the traditional SOR, and therefore the category of evidence, and the
- 38. lowest mean was seen for the recommendation which could not be recommended by the research evidence ie was based solely on expert opinion. This new system has the advantage of allowing the SOR to be upgraded or downgraded based on ex- pert opinion relating to global aspects of health care delivery, such as generalizability, safety, cost- effectiveness and patient preference, and common sense. It therefore gives an additional dimension and weighting to guideline recommendations other than just the support from research evidence alone. In the traditional system, the term ‘strength of recommen- dation’ is almost a misnomer as it directly relates to the category of evidence and provides little extra information beyond that afforded by the ‘category of evidence’. This is an important limitation of currently practised evidence-based guideline methodology that was overlooked in a recent critique of the meth- odology of OA guidelines (Pencharz et al . 2002). During the development of guidelines there are many situations for which the existing SOR method- ology (Shekelle et al . 1999) is not ideal. Interventions
- 39. for which placebo-controlled trials are impractical or unethical (e.g. total joint replacement) cannot score highly on the existing hierarchy and yet clearly may Figure 1 Comparison of mean VAS (95% confidence intervals) and traditional strength of recommendation. VAS, visual analogue scale; NR, not recommended. 0 1 2 3 4 5 6 7 8 9 A C D NR Strength of recommendation (Traditional method) M ea n V A S ( cm
- 40. ) VAS = visual analogue scale, NR = not recommended E. Roddy et al. 350 © 2006 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice , 12 , 3, 347–352 be very efficacious and warrant strong recommenda- tion for clinical practice. The new method allows
- 41. the recommendation for such interventions to be upgraded beyond that afforded by the category of research evidence. Furthermore, when recommenda- tions are not easily assessed in the setting of a clinical trial yet have clear face validity, as with our third and fourth recommendations (Table 2), the panel may feel a much stronger recommendation is warranted than that permitted by the current research-linked method. For example, the mean VAS for both prop- ositions 4 and 5B (Table 2) was 7.7, yet the SOR according to the traditional methodology were D and 1B respectively. This reflects that although proposi- tion 4 would be impractical to assess in the setting of a RCT, it was highly supported by the expert panel Table 2 Evidence-based recommendations for the role of exercise in the management of osteoarthritis of the hip or knee: category of evidence, strength of recommendation (Shekelle et al . 1999) and visual analogue score (VAS) Recommendation Category of Evidence (1–4) Strength of Recommendation (A-D)
- 42. Strength of recommendation (VAS) – Mean (SD) cms 1. Both strengthening and aerobic exercise can reduce pain and improve function and health status in patients with knee and hip OA. Knee 1B Hip 4 A C (extrapolated from knee OA) 8.9 (1.1) 6.3 (2.1) 2. There are few contra-indications to the prescription of strengthening or aerobic exercise to patients with hip or knee OA. 4 C (extrapolated from adverse event data) 8.0 (1.5) 3. Prescription of both general (aerobic fitness training) and local (strengthening) exercises is an essential, core aspect of management for every patient with hip or knee OA.
- 43. 4 D 7.1 (2.5) 4. Exercise therapy for OA of the hip or knee should be individualized and patient-centred taking into account factors such as age, co-morbidity and overall mobility. 4 D 7.7 (1.9) 5. To be effective, exercise programmes should include advice and education to promote a positive lifestyle change with an increase in physical activity. 4 1B D A 6.1 (2.6) 7.7 (1.4) 6. Group exercise and home exercise are equally effective and patient preference should be considered. 1A 4 A D
- 44. 8.0 (1.5) 7.6 (2.3) 7. Adherence is the principal predictor of long-term outcome from exercise in patients with knee or hip OA. 4 D 5.1 (2.4) 8. Strategies to improve and maintain adherence should be adopted, e.g. long-term monitoring/review and inclusion of spouse/family in exercise. 1B A 7.6 (1.5) 9. The effectiveness of exercise is independent of the presence or severity of radiographic findings. 4 Not recommended 4.5 (2.8) 10. Improvements in muscle strength and proprioception gained from exercise programmes may reduce the progression of knee and hip OA. 4 D 4.2 (2.5) Grading strength of guideline recommendations ©
- 45. 2006 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice , 12 , 3, 347–352 351 whereas robust evidence from RCTs exists to sup- port proposition 5B. Finally, the traditional hierarchy does not accommodate the scenario where research evidence contradicts a recommendation, as with our ninth recommendation (Table 2). Other guideline methodology groups have attempted to overcome these limitations and reduce the dependence of the SOR on the category of research evidence. However, the grading systems, produced by American College of Cardiology/ American Heart Association (ACC/AHA) Task Force (ACA/AHA 2004), the US Preventive Services Task Force (2003), the National Institute for Clinical Excellence (NICE) (NICE 2004) and the New Zealand Guidelines Group (New Zealand Guide-
- 46. lines Group 2004), derive the SOR primarily from the category of research evidence. The ACC/AHA guidelines state that any combination of classification of recommendation and level of evidence is possible and that a recommendation can be strongly sup- ported even if it is based entirely on expert opinion and no research studies have ever been conducted on the recommendation (ACA/AHA 2004). However, this system does not provide for the incorporation of factors such as cost-effectiveness and safety, and the descriptive and quantitative criteria for assigning the classification and evidence ratings weight research evidence and clinical expertise equally, which may not be appropriate for some modalities, e.g. total joint replacement. The guideline development methods of NICE state that when the evidence is very strong, this should translate directly into a rec- ommendation, yet when the literature search finds no evidence to answer the clinical question, the guide- line development group should consider using con- sensus methods to identify current best practice, suggesting that consensus methods are only needed when there is no robust evidence (NICE 2004). Furthermore, NICE produces guidance on the role of individual treatments rather than disease-orientated recommendations on global treatment strategies. The recently published GRADE collaboration (Atkins et al . 2004), although highlighting the difficulties in producing clinical guidelines and grading strength of recommendation, has not produced a simple, practi- cal solution. The VAS, on the other hand, has the
- 47. advantage of being simple to apply and allows all facets to be incorporated, e.g. category of research evidence, safety, cost-effectiveness, generalizability and expert opinion. A limitation of the VAS-SOR methodology is that as the basis for the VAS is not based on explicit criteria, it cannot be examined and assessed readily by external groups. However, we recommend that the VAS method should be used alongside the tra- ditional method of determining the category of research evidence supporting each recommendation. Any discrepancy between the category of evidence and SOR would therefore be highlighted and should then be justified in the ensuing discussion. A further limitation is that this method has only been used in the setting of recommendations for exercise in osteoarthritis by a single group of experts, so evi- dence of its generalizability to other fields and other groups is required. Other possible methods for grading SOR include the development of an ordinal scale. A numerical scale, however, is commonly used to assess self- reported pain and disability in clinical trials, and applying this principle to SOR seemed preferable. Although the numerical scale scores themselves do not have intrinsic comparability between different sets of guidelines, there is at least scope for grading or even ranking of different recommendations within each set of guidelines. Other groups that prefer verbal scales may wish to develop an ordinal scale with descriptors to help guide practice in a clinical setting.
- 48. Our guideline development group concludes that, in comparison to existing traditional methodology, this new system of grading SOR is less constrained and offers the advantage of allowing the SOR for procedures which cannot be assessed in RCTs to be upgraded according to expert opinion consistent with the principles of evidence-based medicine (Sackett et al . 1996). We would encourage other groups that develop management recommendations or guide- lines to try this approach, so that its clinical applica- bility and usefulness can be determined more widely. Acknowledgements We are grateful for an educational grant from MOVE (http://www.move.uk.net) and are also indebted to the Arthritis Research Campaign, UK for financial support (ICAC grant D0593; WZ Senior http://www.move.uk.net E. Roddy et al.
- 49. 352 © 2006 Blackwell Publishing Ltd, Journal of Evaluation in Clinical Practice , 12 , 3, 347–352 Lectureship D0565). We would also like to thank Dr Jinying Lin, a visiting scholar from The People’s Hospital of Guangxi Province, China, for assistance with data entry. John Dickson during the past 5 years has received support to attend or organize symposia, or has received a speaker’s honoraria, or a board member’s honoraria from one or more of the following com- panies – MSD, Wyeth, Pfizer, BI, TSB Chemedica, GSK. He has received research funding from Q-med. He has shares in Merck and Pfizer. Marion McMurdo is a Director of D D Develop- ments Limited, a University of Dundee company
- 50. whose mission is to provide exercise opportunities for older people. Profits go to ageing research. References American College of Cardiology/American Heart Associ- ation (2004) Manual for ACC/AHA Guideline Writing Committees. Section II: Tools and Methods for Creating Guidelines. Step Six: Assign Classification of Recommen- dations and Level of Evidence. Available at: http://www.acc.org/clinical/manual/manual_Iistep6.htm (accessed 13 July 2004). Atkins D., Best D., Briss P.A. et al. (2004) Grading quality of evidence and strength of recommendations. BMJ
- 51. 328 , 1490. Dougados M., Betteridge N., Burmester G.R. et al. (2004) EULAR standardised operating procedures for the elaboration, evaluation, dissemination, and implementa- tion of recommendations endorsed by the EULAR standing committees. Annals of the Rheumatic Disease 63 , 1172–1176. Field M. & Lohr K. (1990) Clinical Practice Guidelines: Directions for a New Program . National Academy Press, Washington DC.
- 52. Jordan K.M., Arden N.K., Doherty M. et al. (2003) EULAR recommendations 2003: an evidence based approach to the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Annals of the Rheumatic Disease 62 , 1145–1155. National Institute for Clinical Excellence (2004) Guideline development methods. Chapter 11: creating guideline recommendations. Available at: http://www.nice.org.uk/pdf/GDM_Chapter11.pdf (accessed 13 July 2004). New Zealand Guidelines Group (2004). Grading Systems
- 53. for Guidelines. Available at: http://www.nzgg.org.nz (accessed 13 July 2004). Pencharz J.N., Grigoriadis E., Jansz G.F. & Bombardier C. (2002) A critical appraisal of clinical practice guidelines for the treatment of lower-limb osteoarthritis. Arthritis Research 4 , 36–44. Pendleton A., Arden N., Dougados M. et al. (2000) EULAR recommendations for the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Annals of the Rheumatic Disease
- 54. 59 , 936–944. Roddy E., Zhang W., Doherty M. et al. (2005) Evidence- based recommendations for the role of exercise in the management of osteoarthritis of the hip or knee – the MOVE consensus. Rheumatology 44 , 67–73. Sackett D.L., Rosenberg W.M., Gray J.A., Haynes R.B. & Richardson W.S. (1996) Evidence based medicine: what it is and what it isn’t. BMJ
- 55. 312 , 71–72. Shekelle P.G., Woolf S.H., Eccles M. & Grimshaw J. (1999) Clinical guidelines: developing guidelines. BMJ 318 , 593–596. US Preventive Services Task Force Ratings (2003) Strength of Recommendations and Quality of Evidence. Guide to Clinical Preventive Services , 3rd edn. Periodic Updates, 2000–2003. Agency for Healthcare Research and Qual- ity, Rockville, MD. Available at: http://www.ahrq.gov/clinic/3rduspstf/ratings.htm
- 56. (accessed 13 July 2004). Zhang W., Doherty M., Arden N. et al. (2004) EULAR evidence-based recommendations for the management of hip osteoarthritis – report of a task force of the Stand- ing Committee for International Clinical Studies Includ- ing Therapeutic Trials (ESCISIT). Annals of the Rheumatic Disease. Published Online First: 7 October 2004, 10.1136/ard.2004.028886. http://www.acc.org/clinical/manual/manual_Iistep6.htm http://www.nice.org.uk/pdf/GDM_Chapter11.pdf http://www.nzgg.org.nz http://www.ahrq.gov/clinic/3rduspstf/ratings.htm