This document discusses the development of quality standards for colposcopy education, training, and practice in Europe from 2010-2019. It summarizes discussions and consensus reached at several European Federation of Colposcopy (EFC) satellite meetings and congresses regarding:
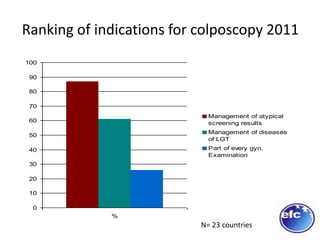
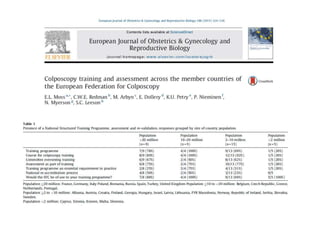
1) The status of colposcopy education/training and how colposcopy is practiced across Europe.
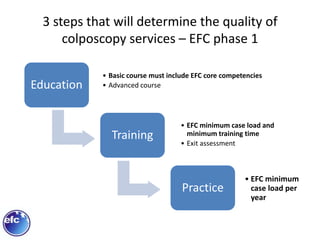
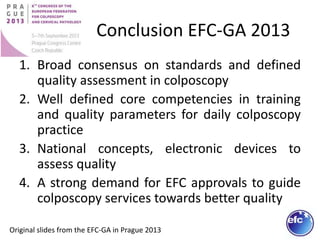
2) Developing European standards for colposcopy including minimum requirements for training programs, case loads for trainees/practitioners, and qualifications for trainers.
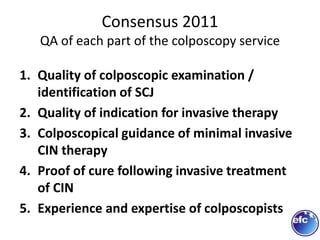
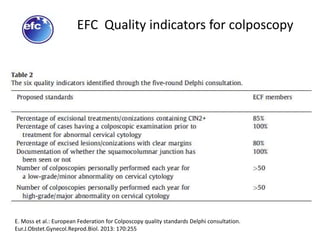
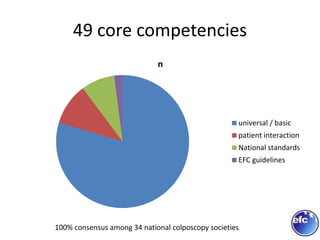
3) Reaching consensus on core competencies for colposcopy training and quality indicators for colposcopy services through repeated Delphi studies involving EFC member countries.























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

