

Recommended
Recommended
More Related Content
Similar to GERD.pdf
Similar to GERD.pdf (20)
More from عباس مشتاق
More from عباس مشتاق (19)
Recently uploaded
Recently uploaded (20)
GERD.pdf
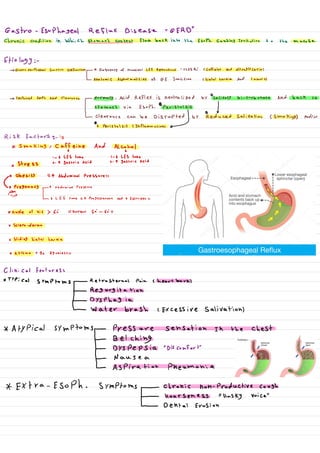
- 1. Gastroesophageal flux DiseaseRessoph. causing irritation to the masae Etiology:- -> Gastroesophageal Junction Dysfunction - ↑ Frequency of transient LES Relaxations " TLESR,"(Caffeine And Nitroglycerin) LanatomiC Abnormalities of of Junction Chiatal hernia And tumors) - > Impaired Esoph. Acid Clearance - Normally, Acid Reflex is neutralized by salivary bi-carbonate and back to Lstomach via Esoph. O peristalsis ↓ pearance,canbedisrupted by reduced Salination (smokings andare S Risk factors- is * smoking, caffeine And Alcohol A 1 - 6 LES tone 1- 6 LES tone x stress -- A gastric Acid 2- ↑ gastric Acid x obesity ↑ Abdominal Pressures * Pregnancy ↑ Abdominal Pressure -I - Lo LES fone 4 Progesterone And 4 Estrogen *Angle of his 6: normal 50-60 X Sclero-derma x sliding hiatal hernia * Asthma B2 Agonists Clinical features: * Typical symptoms - Retrosternal Pain (heartburn) ↓ Regurgitation - _ ° Dysphagia L water brash, excessive salivations * Atypical symptoms - Pressure sensation in the chest ↓ Belching - DYSPCPSia "Discomfort" L Nause a - ↳ Aspiration Pheumonia * Extra-Esoph. symptoms - chronic non-productive cough I Hoarseness Husky voice" - Dental Erosion
- 2. Aggravating factors: - ~ Ling Down shortly After meals * certain foods/beverages Red flags 8 Anemia And/or GS Bleeding" hematemesis, hematochezia " 0 weight loss o vomiting * Male ·Presence of 71 Risk for Barrett esoph. *rees, soy ~ obe se * SYMP1oms>5Y * European Decent Diagnosis:- - There is no gold standard test for the Dx of GERD. - If Patient with chest pain -> ECG + Cardiac Enzyme "troPonin" -> Normal - Patient with suspecte GERD Without Red flags or high Risk of Barrett Esoph. Start with once-Daily PPI for 8 * If relief symptoms of GERD - can stop PPI * If Persist symptoms or Recur After stop PPI or Red flags or High Risk for Barrett ESOPL. -> E6D A esoau. Monitoring * If Erosive will see by ↳ measure so. PH over 24-48 h using telemetry capsule catheter - PH -> Abnormal "Nor-crosise Reflux Disease" I X treat by PPI for 8 W - With Normal EGD And PH treat by Low Dose PPI or H2 Antagonists -I
- 3. ↑ reatment :- * Initial with lifestyle changes And Acid suppression therapy ppy, Hz Antagonist. * Surgical therapy" is not Routinely indicated"(fundoplication() 18: Dor fundo. !27 Toupet fundo. 360 complete fund. "Nissen fundoplication" complication.. B arrett Esophages "Intestinal metaplasia of the ESOPL. mucosa IDA - mucosal erosion and ulceration - Chronic Bleeding- Anemia Esophageal stricture = SoPhageal Ring "Schatzki Rings" Aspiration pneumonia Reflux laryngitis Hoarsenesss) * St -