Abdominal Examination .pdf
•
2 likes•266 views

Explained of abdominal examination including inspection, palpation, percussion and auscultation

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Abdominal Examination .pdf
Similar to Abdominal Examination .pdf (20)
More from عباس مشتاق
More from عباس مشتاق (19)
Recently uploaded
Recently uploaded (20)
Abdominal Examination .pdf
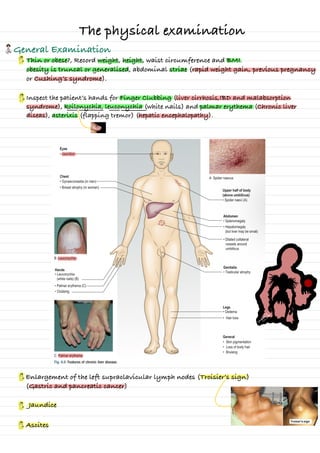
- 1. The physical examination General Examination Thin or obese?, Record weight, height, waist circumference and BMI. obesity is truncal or generalised, abdominal striae (rapid weight gain, previous pregnancy or Cushing’s syndrome). Inspect the patient’s hands for Finger Clubbing (liver cirrhosis,IBD and malabsorption syndrome), koilonychia, leuconychia (white nails) and palmar erythema (Chronic liver diseas), asterixis (flapping tremor) (hepatic encephalopathy). Enlargement of the left supraclavicular lymph nodes (Troisier’s sign) (Gastric and pancreatic cancer) Ascites Jaundice ⑮missionate ⑮i winsse ⑱ . . . . . . . . . insane ⑮instantia ⑮missionse ⑮missionate
- 2. Abdominal Examination Pt. In Supine Position with pillow under the head to relax the abdominal wall muscles. Inspection 1- From End of Bed • look for any Abdominal Distention (Ascites, Intestinal obstruction) or Mass (abdomen Extending or Not; Symmetry “Both side Move Above and Below During inspiration and expiration “ or Asymmetry. 2- From Rt. Side • Visible veins (portal hypertension or vena cava obstruction) • Skin In older patients (Campbell de Morgan spots) are common and normal, striae, bruising, Rash. • Abdominal scars and stomas or Mass • Tube Drain • Visible Pulsation (AAA “aortic abdominal aneurysm”, Mass)and peristalsis • Hair Distribution 3- Bird View • The umbilicus is usually inverted • Umbilical at the level of the iliac crests if Rise (pregnant) down (ascites) • umbilical hernia is a distended and everted umbilicus and may have a palpable cough impulse Expose the abdomen from the nipple to mid thigh or from the xiphisternum to the symphysis pubis • Ask Pt. To Cough or valsalva Maneuver for any Bulging & 3 Sig sy 12 2
- 3. Palpation • Ensure your hands are warm and clean • Ask the patient to any pain and to report any tenderness during palpation • Observe the patient’s face throughout for any sign of discomfort 1- superficial palpation • Tenderness EG PUD; RH cholecystitis; LIF diverticulitis; RIF appendicitis or Crohn’s ileitis) • Masses 2- Deeper palpation • Rebound tenderness (for area with tenderness in superficial palpation • Describe any mass • Enlarged organs (liver, gallbladder “Acute cholecystitis” (Murphy’s sign), spleen and kidneys in turn during deep inspiration. • guarding • Rovsing’s sign (Acute appendicitis) 1- Site 2- Size 3- Surface (smooth or irregular or Nodular) 4-Shape (Regular or Irregular) 5- Consistency (Soft or Hard) 6- Moves on respiration 7- Fixed or mobile 8- Deep “intra-abdominal” or superficial 9- Mass is an enlarged abdominal organ or separate from the solid organs) a gastric or pancreatic tumour or an aortic aneurysm, metastatic cancer (‘Sister Mary Joseph’s nodule’). As the patient takes a deep breath in, gently palpate in the right upper quadrant of the abdomen; the acutely inflamed gallbladder contacts the examining fingers, evoking pain with the arrest of inspiration Palpation in the left iliac fossa produces pain in the right iliac fossa &
- 4. 1- Place your hand flat on the skin of the right iliac fossa 2- Ask the patient to breathe in deeply through the mouth 3- Move your hand progressively up the abdomen, 1 cm at a time, between each breath the patient takes, until you reach the costal margin or detect the liver edge. Hepatomegaly Palpation Percussion • Ask the patient to hold their breath in full expiration • Percuss downwards from the Rt. 5th or 2nd ICS and mid-clavicular line (dullness indicating upper border of the liver • Measure the distance in from the upper border of dullness to the palpable liver edge • In the normal abdomen, the liver edge below the right costal margin Splenomegaly • Place your hand over the patient’s umbilicus or RIF, ask the patient to inhale deeply through the mouth. • Move your hand diagonally upwards towards the left hypochondrium, 1 cm at a time between each breath the patient takes • If you cannot feel the splenic edge, palpate with your right hand, placing your left hand behind the patient’s left lower ribs and pulling the ribcage forward Palpation Percussion • Percuss over the lateral chest wall • Dullness to percussion posterior to the left mid-axillary line beneath the 9th–11th ribs. ⑱ in e & Early ⑱ ascanin & & SLE
- 5. Ascites Percussion 1- Shifting dullness • With the patient supine, percuss from the midline out to the flanks, Keep your finger on the site of dullness in the flank and ask the patient to turn on to their opposite side. • Pause for 10 seconds to allow any ascites to gravitate, then percuss again. If the area of dullness is now resonant, shifting dullness is present, indicating ascites. Fluid Thrill (Fluid wave test) Cause of Ascites • Splenic vein thrombosis • Portal vein thrombosis • Cirrhosis • Alcohol liver disease • Liver metastases • Right heart failure • Nephrotic syndrome • TB Auscultation • ileocecal valve • 2 Renal A. • 2 iliac A. • 2 Femoral A. • Hepatic hum • Abdominal Aorta 1- Abdominal Examination (Geeky) • https://youtu.be/PYAnF6GJY2I 2- Abdominal Examination (Uo Leicester) • https://youtu.be/SBgWtboujnU 3- Rebound Tenderness • https://youtu.be/1weCV9pGqFM ⑱ in e & & Sinceinthe