Mitral Stenosis
•Download as PPTX, PDF•
3 likes•489 views

Mitral stenosis in pregnancy- pathophysiology & anaesthetic management

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Mitral Stenosis
Similar to Mitral Stenosis (20)
More from Souvik Maitra
Recently uploaded
Recently uploaded (20)
Mitral Stenosis
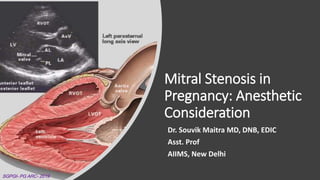
- 1. Mitral Stenosis in Pregnancy: Anesthetic Consideration Dr. Souvik Maitra MD, DNB, EDIC Asst. Prof AIIMS, New Delhi SGPGI- PG ARC- 2019
- 2. “Mitral stenosis may be concealed under a quarter of a dollar. It is the most difficult of all heart diseases to diagnose.” - Sir William Osler SGPGI- PG ARC-
- 3. Chief Complains • 27y female, G2 P1, village dweller, presented at 39 week of amenorrhea with progressive shortness of breath and palpitation for last 4 months • Scheduled for elective LSCS SGPGI- PG ARC-
- 4. HoPI • Shortness of breath- insidious in onset at around 22 wk of amenorrhea, gradually progressing, without any seasonal variation, initially exertional, now patient c/o SOB with ordinary activity. • Palpitation- Occasional, increased with activity • No h/o hemoptysis • No h/o similar illness in the past • No history suggestive of acute rheumatic fever in the past SGPGI- PG ARC-
- 5. Physical Examination • Built & nutrition- average • BMI 22 • BP 100/70, low volume regular pulse, PR 86/min • Bi pedal edema + • Raised JVP • Right parasternal heave + • S1- loud, P2- loud • Mid- diastolic murmur in the mitral area • PA- 38 week of gestation SGPGI- PG ARC-
- 6. What is the clinical diagnosis? •27y female at 39 week gestation with mitral stenosis with pulmonary hypertension in sinus rhythm. SGPGI- PG ARC-
- 7. How will you confirm diagnosis? • 2D Echocardiography with Doppler • Valve area (normal 4-6 cm2) • Transvalvular pressure gradient • LA dimension • PA pressure • RV function • Presence of LA clot • Any other valvular lesion SGPGI- PG ARC-
- 8. Assessment of severity How mitral stenosis is classified? SGPGI- PG ARC-
- 9. Clinical staging of MS ACC/ AHA 2014 What are the stages of MS? SGPGI- PG ARC-
- 10. How to classify dyspnea? NYHA Classification • Class I - No symptoms and no limitation in ordinary physical activity, e.g. shortness of breath when walking, climbing stairs etc. • Class II - Mild symptoms (mild shortness of breath and/or angina) and slight limitation during ordinary activity. • Class III - Marked limitation in activity due to symptoms, even during less-than-ordinary activity, e.g. walking short distances (20- 100 m).Comfortable only at rest. • Class IV - Severe limitations. Experiences symptoms even while at rest. Mostly bedbound patients. SGPGI- PG ARC- 2019 SGPGI- PG ARC-
- 11. Final diagnosis • 27y old term pregnant woman at 39 week of gestation with singleton live fetus with severe mitral stenosis (valve area 0.9 cm2), moderate pulmonary hypertension (PA pressure 40 mm Hg) , in sinus rhythm currently NYHA III scheduled for elective LSCS. SGPGI- PG ARC-
- 12. What are the causes of MS? • Rheumatic heart disease • LA myxoma • Congenital • IE with large vegetations • SLE, RA • Mitral annular calcification ~50% of all rheumatic MS patients don’t have a history of rheumatic fever in childhood. SGPGI- PG ARC-
- 13. Epidemiology • Isolated MS- 40% of all RHD • MS with MR- 40% of all RHD • Rest 20% are multivalvular lesion • Onset of symptoms- 4th decades of life (in Western countries) • Usually 2nd or 3rd decades- in India SGPGI- PG ARC-
- 14. Alteration in CVS examination in pregnancy • JVP- Normal/ raised • Carotid pulse- Normal volume • Peripheral pulse- Well filled • Apex beat- Crisp, displaced superiorly, laterally • S1- Loud, widely split (early closure of mitral valve) • S2- unchanged • S3- May be heard • RV pulsation may be palpable in thin build women • Newmurmursareheardinmorethan90%ofpregnantwomen SGPGI- PG ARC-
- 15. Mitral Stenosis: Clinical features • Progressive dyspnea • Palpitation • Fatigue/ syncope • Embolism- Stroke/ AMI • Hemoptysis • Persistent cough • Left RLN palsy • Edema/ ascites/ hepatomegaly SGPGI- PG ARC- Ortner Syndrome
- 16. What are the findings in general survey in patients with MS? •Malar flush- ‘mitral facies’ •BP- Usually low normal •Peripheral pulse- low volume/ irregularly irregular •Pedal edema - (?RVF/ ? normal in pregnancy) •Build & nutrition- May be under-nurished SGPGI- PG ARC- Uncommon in Indian patients
- 17. What are the classic findings in CVS examination: Inspection • Raised JVP • Visible thrill in the mitral area- may be seen in thin built patients SGPGI- PG ARC-
- 18. •Tapping apex beat •Right parasternal heave •Palpable P2 •Palpable diastolic thrill in mitral area What are the classic findings in CVS examination: Palpation SGPGI- PG ARC-
- 19. •S1- sharp, short & accentuated •Low pitched, mid- diastolic rumbling murmur in the mitral area with presystolic accentuation •OS- high pitched, just after S2 •Loud, narrow split P2 What are the classic findings in CVS examination: Auscultation SGPGI- PG ARC-
- 20. Why there is pre systolic accentuation? “Atrial Kick” Increased flow across MV at end-diastole Accentuation of murmur before systole Patients must be on sinus rhythm SGPGI- PG ARC-
- 21. How the auscultatory findings change with severity? SGPGI- PG ARC- Severe MS Higher pressure gradient between LA & LV Early opening of MV
- 22. What are the D/D of mid- diastolic murmur? Mitral stenosis Tricuspid stenosis (rarely associated with rheumatic MS) ASD with increased flow across tricuspid valve Ball- valve LA thrombus LA myxoma MR causing increased flow in MV Austin flint murmur SGPGI- PG ARC-
- 23. What happens to the JVP waves in MS? • Large a- wave when RA pressure is elevated • Loss of a- wave in AF • Large v wave or c-v wave when there is TR SGPGI- PG ARC-
- 24. What are the typical ECG features in MS? Bifid P wave- ‘P mitrale’ RAD RVH AF Second half of ‘P” wave may be taller Negative 2nd half P in V1 QRS is POSITIVE (dominant R wave) in Lead II, Lead III and aVF QRS is NEGATIVE (dominant S wave) in Lead I 1. RAD 2. Dominant R wave in V 1 3. Dominant S wave in V5/V6 4. QRS duration <120 ms SGPGI- PG ARC-
- 25. What are the ECG features in Afib? • Irregularly irregular rhythm. • No P waves. • Absence of an isoelectric baseline. • Variable ventricular rate. • QRS complexes usually < 120 ms • Fibrillatory waves may be present and either fine (amplitude < 0.5mm) or coarse (amplitude >0.5mm). SGPGI- PG ARC-
- 26. How will assess cardiovascular risk in this patient? SGPGI- PG ARC-
- 27. What is the WHO classification of maternal cardiac diseases? SGPGI- PG ARC-
- 28. What are the pathological changes in mitral valve? SGPGI- PG ARC-
- 29. SGPGI- PG ARC- SGPGI- PG ARC-
- 30. SGPGI- PG ARC-
- 31. What is shape of PV curve in MS? SGPGI- PG ARC-
- 32. How mitral stenosis is different in pregnancy? SGPGI- PG ARC-
- 33. What are the cardiovascular change in pregnancy? • Cardiac output increases up to 50% • Stroke volume increases 20- 30% • Heart rate increased by 10- 15% • Blood volume increases by 40- 45% • SVR decreases throughout pregnancy ~5-10% • Mean systemic filling pressure increases SGPGI- PG ARC-
- 34. Why parturient with MS decompensates? SGPGI- PG ARC- 2019 SGPGI- PG ARC-
- 35. SGPGI- PG ARC- SGPGI- PG ARC-
- 36. MS & pregnancy outcome • 67% pregnant women in severe MS develop significant cardiac events • IUGR/ IUFD- around 40% untreated cases • Pregnant women with MVA<1.5 cm2 usually become symptomatic- even if they are asymptomatic before pregnancy Usually NYHA status degrades one stage in pregnancy SGPGI- PG ARC-
- 37. Principles of medical management • Anticoagulation • Ventricular rate control • Maintenance of sinus rhythm • Diuresis • Bed rest- particularly important in pregnancy SGPGI- PG ARC-
- 38. Anticoagulation Anticoagulation with VKA in MS with AF (paroxysmal/ persistent/ permanent) LA thrombus Prior embolic/ thrombotic events SGPGI- PG ARC-
- 39. Anticoagulation in Pregnancy • SC/IV heparin for up to 12 weeks antepartum (aPTT 1.5–2.5-times of normal) • Warfarin from 12 to 36 weeks (maintain INR 2.5–3.0) • SC/IV heparin after 36 weeks • LMWH is preferred over UFH • Anti factor X-a level monitoring is recommended in pregnancy SGPGI- PG ARC-
- 40. How safe are the anticoagulants in pregnancy? • Warfarin- Risk of embryopathy, miscarriage & hemorrhage C/I in first & third trimester UFH/ LMWH- does not cross placenta Higher dose of UFH/LMWH required UFH to be discontinued at least 6h before LSCS/ induction of labor LMWH to be discontinued 12h before LSCS/induction of labor Higher plasma volume Higher renal clearance Metabolism by placental heparinase SGPGI- PG ARC-
- 41. Rate & rhythm control in pregnancy • Beta blocker- Metoprolol/ Atenolol- ? Fetal growth restriction • Calcium channel blocker- Verapamil may be used • Digoxin- unreliable effects in pregnancy SGPGI- PG ARC-
- 42. Diuretics in pregnancy • Furosemide, bumetanide, hydrochlorothiazide- can be used • Maternal hypovolemia to be avoided- risk of low cardiac output • Oligohydramnios & fetal dys-electrolytemia can occur The BMJ 2018 SGPGI- PG ARC-
- 43. MS with AF with unstable hemodynamics? •Cardioversion is the choice •Safe to the fetus at all trimester •Transient fetal bradycardia- fetal monitoring required •IV heparin- when AF is for more than 48h SGPGI- PG ARC-
- 44. Intervention in Pregnancy • Percutaneous mitral balloon commissurotomy is reasonable for pregnant patients with severe MS (mitral valve area ≤1.5 cm2, stage D) with valve morphology favorable, who remain symptomatic with NYHA class III to IV HF symptoms despite medical therapy. • Preferably be performed after 20 weeks of gestation • Presence of LA thrombus is a contraindication ACC/ AHA 2014 SGPGI- PG ARC-
- 45. What is favorable valve morphology? • A mitral valve with a score <8 to 9 with no more than moderate mitral regurgitation is deemed the best candidate for PBMV. SGPGI- PG ARC-
- 46. Does surgery have any role? • Surgical commissurotomy- Carries high fetal risk (2- 10%) • MV replacement (CPB)- Risk of fetal loss may be up to 20- 30% Maternal risk 2-8% • Patients with severe MS should undergo intervention before pregnancy SGPGI- PG ARC-
- 47. Obstetric Management SGPGI- PG ARC-
- 48. Vaginal birth vs LSCS • “Vaginal delivery, with epidural analgesia, is preferred for the majority of women. Invasive monitoring should be used in symptomatic women and those with severe MS. ” RCOG 2006 SGPGI- PG ARC-
- 49. Vaginal birth vs LSCS • Mild MS, and in patients with moderate or severe MS in NYHA class I/II without pulmonary hypertension- Vaginal delivery • Moderate or severe MS who are in NYHA class III/ IV or have pulmonary hypertension despite medical therapy- LSCS can be considered SGPGI- PG ARC- ESC 2011
- 50. Hemodynamics during normal labor SGPGI- PG ARC-
- 51. Goals during vaginal delivery •Second stage of labor to be curtailed •Avoid pain & sympathetic stimulation •Epidural analgesia is desirable •Assisted delivery is the choice SGPGI- PG ARC-
- 52. Labor analgesia in mitral stenosis • Low conc. LA with opioid in epidural • IT opioid with low conc. LA in epidural (CSE) can be used • IT opioid (fentanyl 25mcg) can be used as sole agent • Carefully titrated- avoid sudden vasodilatation • Epinephrine test dose- Avoid • FHR monitoring is mandatory • Goal is to avoid tachycardia & maternal bear down effort Valsalva maneuver Increased venous return Increased CO Increased MV flow Increased LA pressure Increased pulm v. pressure SGPGI- PG ARC-
- 53. Anesthetic management SGPGI- PG ARC-
- 54. Preoperative investigations • Hemogram • Electrolytes (because patients often receive diuretics) • 12 lead ECG • 2D Echocardiography with Doppler • Coagulation profile (Ptime?/ aPTT?) SGPGI- PG ARC-
- 55. What monitoring will you use? • 5-lead ECG • SpO2 • NIBP • IBP • EtCO2 • CVP? SGPGI- PG ARC-
- 56. What is the choice of anesthetic technique? • General anesthesia, spinal anesthesia, epidural anesthesia & combined spinal epidural anesthesia- all have been used • Choice of anesthetic technique depends upon clinical condition of the patients SGPGI- PG ARC-
- 57. Anesthetic Goals • Heart rate- Avoid tachycardia (60- 70 bpm), maintain sinus rhythm • Preload- ‘Optimum’ • Afterload- Not to be reduced (SBP/ MAP to be maintained within 20% of baseline) • Contractility- To be maintained • Decrease PVR LA pressure Cardiac output ⬇️ SVR ~ CO ⬇️ DBP ⬇️ CPP SGPGI- PG ARC-
- 58. What drug to be used for RV failure? • Milrinone is the drug of choice • Typical dose is 50 mcg/kg loading by IV over 10 minutes, then 0.375-0.75 mcg/kg/min IV • Noradrenaline at low dosage may be needed to counteract hypotension SGPGI- PG ARC-
- 59. Sub- arachnoid block • Single injection SAB not recommended in severe MS- risk of sudden fall in SVR • Low dose SAB (1.2ml- 1.5ml) has been used in mild to moderate cases. • Boluses of phenylephrine (40- 100 mcg)- for counteracting hypotension & fall in SVR • Continuous spinal catheter- option for titration SGPGI- PG ARC-
- 60. Epidural anesthesia • Can be titrated, • Slow onset- maternal cardiovascular system may be ‘adapted’ • May be associated with less hemodynamic perturbation • Larger volume of LA required • Can’t be used in emergency scenario SGPGI- PG ARC-
- 61. Combined spinal- epidural anesthesia • Faster onset of block • Quality & duration of block can be increased subsequent epidural LA injection. • 5- 6 mg 0.5% heavy bupivacaine can be used • Epidural supplementation can be provided by 2-3 ml boluses of LA • Provides excellent postoperative analgesia • Epidural volume expansion by NS can achieve higher block SGPGI- PG ARC-
- 62. General anesthesia: Indications • Patients with ‘critical MS’ • Patients with pulmonary edema • Patients on LMWH/ UFH • Patients who can’t tolerate supine position SGPGI- PG ARC-
- 63. How will you provide GA in this patient? Induction of general anesthesia Avoid Ketamine- Tachycardia Propofol- Cause decrease in SVR & hypotension Thiopentone- Cause myocardial depression Etomidate- Provides stable maternal hemodynamics Prevent laryngoscopy & intubation responses IV lignocaine IV esmolol IV short acting opioid: Remifentanil (0.5 mg/kg) is choice, fentanyl (1- 2 mcg/kg) can be considered- Neonatology team must be informed Avoid tachycardia Avoid vasodilatation Avoid hypoxia, hypercarbia SGPGI- PG ARC-
- 64. Maintenance of anesthesia •Nitrous oxide should be avoided if PAH is a concern •Potent inhalation anesthetics are choice (isoflurane/ sevoflurane)- Risk of uterine atony •Intermediate acting NM blockers are used SGPGI- PG ARC-
- 65. Reversal of GA • Extubation response must be prevented • Avoid tachycardia • Hypoventilation/ hypoxia to be avoided • Post of pain management is of vital management (Postop epidural opioid, TAP block) SGPGI- PG ARC-
- 66. Fluid & hemodynamics management • IV fluid to be optimized- prevent pulmonary edema. • Baby delivery causes auto-transfusion of 500- 700 ml of blood • Post spinal hypotension to treated by boluses of phenylephrine (25– 100 mcg) • Phenylephrine infusion can also be considered (0.75- 2 mcg/kg/min) • Avoid beta stimulant drugs (ephedrine/ mephentermine) SGPGI- PG ARC-
- 67. How will you guide fluid therapy? • CVP- Not a predictor of LA pressure • Acute rise of CVP indicates RV dysfunction • PCWP is usually overestimates LA pressure • PA catheter can derive SV, SVR & PVR SGPGI- PG ARC-
- 68. Postoperative Hemodynamics SGPGI- PG ARC-
- 69. Postoperative pain management • Postoperative pain management is of paramount importance- multimodal analgesia • B/L USG guided TAP block • Intrathecal morphine (LD:50- 100 mcg/ HD:150- 250 mg) • Epidural morphine/ oxycodone • Surgical site LA infiltration SGPGI- PG ARC-
- 70. Thank You!
Editor's Notes
- TEE & cardiac catheterization may be required for formulation of management plan- before PMBC (to exclude LA thrombus, MR) Cardiac cath – when there is large discrepancy between Doppler & clinical symptoms
- Mitral stenosis is almost always rheumatic even if there is no history of rheumatic fever in childhood
- prominent A wave in sinus rhythm, unless AF (tall c-V wave) or PHTN - lost of x decent, RV failure (Kussmaul…)
- Loud S1- excursion of mobile mitral leaflets against pressure gradient Soft S1- immobile MV- may be associated with MR OS- due to sudden doming of MV in ventricle, best heard just medial to the apex Narrow split- b/o pulm. HTN
- A longer duration of murmur- more to time to flow- more stenosis
- fluttering, distortion, and early closure of the AMVL caused by the aortic regurgitant jet may play a role in the Austin Flint murmur.
- P- mitrale Negative 2nd half P in V1 RAD- QRS is POSITIVE (dominant R wave) in Lead II, Lead III and aVF QRS is NEGATIVE (dominant S wave) in Lead I
- Cardiac catheterization is only required when 2D Echo and Doppler findings are not concordant with the clinical symptoms. LA- LV gradient PCWP usually overestimates LA pressure
- Smaller & shifted leftwards
- Although the physiologic changes in the cardiovascular system appear to begin in the first trimester, these changes continue into the second and third trimesters, when the cardiac output increases by approximately 40% of the pre-pregnant values. The cardiac output increases from the fifth week of pregnancy and reaches its maximum levels by 32 weeks.
- The increased heart rate of pregnancy limits the time available for left ventricular filling, resulting in increased left atrial and pulmonary pressures and an increased likelihood of pulmonary oedema. When the pulmonary capillary pressure exceeds the blood oncotic pressure, pulmonary oedema develops. Pregnancy is also a hypercoagulable state- more thrombosis
- Warfarin- embryopathic at first trimester Fetal hemorrhage May be safe at lower dose, <5mg/day Neither unfractionated heparin (UFH) nor low-molecular-weight heparin (LMWH) crosses the placenta and both are considered safe in pregnancy. Furthermore, LMWH has a better safety profile, with fewer side effects such as thrombocytopenia, bleeding and osteoporosis.
- Calcium channel blocker use in the third trimester was associated with increased risk of neonatal seizures, jaundice, and hematologic disorders
- Another indication systolic PAP > 50 mm Hg (ESC)
- In patients undergoing mitral valvuloplasty for mitral stenosis, an echocardiographic scoring system based on 1) leaftlet mobility, 2) valve thickening, 3) calcification, 4) subvalvular thickening can be used to predict the procedural outcome. Each item is graded from 1 (normal) to 4 which yield a score from 4 to 16. A score of 8 or less predicts a more favorable outcome than those with a higher score. However, a score higher than 8 does not exclude a patient from having a mitral valvuloplasty.
- ECC recommendation
- During the second stage of labour, only the uterine contractile force should be allowed rather than the maternal expulsive effort that is always associated with the valsalva maneuver.
- IBP- may not be required in mild MS cases CVP- does not actually reflect LA preload. Role is controversial. Useful when use of inotropes are necessary. Acute rise in CVP denotes RV dysfunction TEE may be used in major surgery e.g major GI surgery etc.
- Rapid heart rate shortens diastolic filling time, increases the left atrial pressure and the pulmonary venous pressure and causes heart failure symptoms. Afterload reduction is always associated with some preload reduction Usually LV contractility is maintained in isolated MS- there may be some fibrotic changes in postero-basal region of LV
- At a dose of 1 μg/kg, remifentanil prior to induction of general anaesthesia increases the risk of neonatal respiratory depression during first minutes after caesarean delivery but duration of clinical symptoms is short.
- The sudden increase in the pre-load immediately after delivery, due to autotransfusion from the uterus, may flood the central circulation, resulting in severe pulmonary oedema. In addition, there continues to be autotransfusion of blood for 24–72 h after delivery. Thus, the risk of pulmonary oedema extends for several days after delivery. The greatest risk occurs in the peripartum period, and most deaths occur between the second and ninth days post-partum.
- LD: Shorter duration of analgesia (around 4.5h shorter), less pruritus & PONV Epi Oxycodone: less pruritus, inferior analgesia, compared to morphine