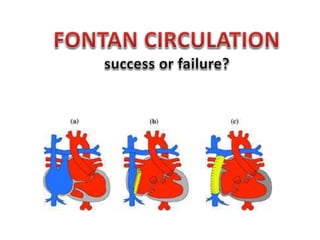
Fontan circulation
•
56 likes•6,865 views

- The document discusses the Fontan procedure for univentricular heart defects. It covers the evolution of the Fontan concept from the original atriopulmonary connection to lateral tunnel and extracardiac conduit techniques. It also discusses indications for Fontan, complications such as arrhythmias and ventricular dysfunction, and strategies to optimize outcomes like fenestration.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Fontan circulation
Similar to Fontan circulation (20)
More from Shivani Rao
More from Shivani Rao (12)
Recently uploaded
Recently uploaded (20)
Fontan circulation
- 2. CONTENT OF DISCUSSION • Introduction • The ‘Fontan’ concept • Indications for Fontan Operation • Fontan physiology • Evolution of Fontan Operation • Fenestration • Post Fontan Complications (Failing Fontan) • Post-op follow up Outcomes • Conclusion
- 3. Introduction • “So in whatsoever creature there is lungs, there is likewise in them two ventricles of the heart, the right and the left” William Harvey (1628)
- 4. Introduction • Normal mammal cardiovascular system • Double—pulmonary and systemic—circuit, connected in series • Powered by double pump—‘‘right’’ and ‘‘left’’ heart. • Many Cardiac malformations ( prevalence approximately 1 per 3000 births) are characterised by only one functional ventricle. • Fontan surgery is performed as the final staged operation not amenable to biventricular repair.
- 7. Modifications of fontan Original fontan 1971 Kreutzer 1973 Bjork1979 Kawashima 1983 Lateral tunnel Extra cardiac condu
- 9. INDICATION FOR FONTAN (UNIVENTRICULAR REPAIR) Absence of two adequate AV valves • Tricuspid atresia / Mitral atresia / Hypoplastic left heart • AV canal defects with atresia or straddling of one AV valve Two adequate AV valves with one hypoplastic ventricle • Double inlet LV / RV • Straddling of one AV valve Repair possible but incomplete or difficult • Large / multiple / non routable VSDs • Miscellaneous • PA with IVS • Heterotaxy syndromes
- 10. Ten Commandments • AGE – 4 to 15 years • NSR • Normal SV Drainage • Normal RA Volume • Adequate PA size ( PA > 0.75 of Aorta) • Mean PAP <15 mmHg • PVR < 4 Woods units • Normal LV Function • Absence of pulmonary artery distortion • Competent AV Valve Chousset et al 1977 Ideal candidate 1978, Choussat et al
- 11. Ten Commandments (or Four !) • AGE – 4 to 15 years (>2 years) • NSR (Atrial Pacing) • Normal SV Drainage (Kawashima repair) • Normal RA Volume (ECTC, RA plasty) • Adequate PA size ( PA > 0.75 of Aorta) • Mean PAP <15 mmHg • PVR < 4 Woods units • Normal LV Function • Absence of pulmonary artery distortion (PA plasty) • Competent AV Valve (AV Valve repair) Ideal candidate
- 12. • Only two significant risk factors for both early and late outcomes • Preoperative ventricular function • Preoperative pulmonary artery pressures >15 mmHg. • Can be viewed as relative contraindications for Fontan
- 14. Normal PhysiologyUniventricular HeartFontan Physiology Marc Gewillig Heart 2005;91:839–846.
- 15. Fontan Circulation • The systemic venous return enters the pulmonary circulation, without an interposing ventricle, and • All shunts at the venous, atrial, ventricular and arterial level are interrupted • Thus places the systemic and pulmonary circulations in series driven by a SV • post capillary energy - no longer wasted in systemic veins, but collected and used to push blood through lungs
- 16. • Advantages of a Fontan circuit : – (near) normalisation of the arterial saturation – abolishment of chronic volume overload on SV • Cost for such circulation : – Chronic systemic venous hypertension and congestion – decreased cardiac output, both at rest and during exercise • Cardiac output - no longer determined by heart, but by the transpulmonary flow (in turn regulated by PVR)
- 17. Fontan Circulation Hemodynamics Caval venous pressure drives pulmonary blood flow Fontan Paradox!! Normal circulation: Pulmonary artery pressure >15 mm of Hg, caval venous pressures < 10 mm of Hg Fontan circulation: Caval venous pressure is > 10 mm Hg and pulmonary artery pressure is less than 15 mm HG Fontan circulation imposes caval hypertension and pulm arterial hypotension
- 18. Cardiac Output in Fontan • No pulsatile pump to add forward energy to flow through lungs • Flow return from the pulmonary vascular bed is thereby restricted • Decreased or absent preload reserve to the ventricle. • Cardiac output (and thus preload) in a Fontan circulation at rest is decreased to 70% (range 50–80%) of normal Marc Gewillig et al. Interactive CardioVascular and Thoracic Surgery 10 (2010) 428–433
- 19. Determinants of Cardiac Output Contractility Heart Rate Preload/Afterload
- 20. Role of Contractilty • Does not Play significant role in Fontan Patients • Except in Severe ventricular dysfunction • In normal ventricular Function under filling is biggest problem Marc Gewillig et al. Interactive CardioVascular and Thoracic Surgery 10 (2010)
- 21. Role of Heart Rate Plays Negligible role Tachycardia does not increase cardiac output Chronotropic incompetence AV synchrony is important Marc Gewillig et al. Interactive CardioVascular and Thoracic Surgery 10 (2010) 428–433
- 22. Role of Preload • Most important determinant • Determined by transpulmonary flow and fenestration • Transpulmonary flow determined by – Transpulmonary gradient ( Venous pressure / LAP) – Transpulmonary resistance (Fontan Resistance / PVR)
- 23. Transpulmonary gradient Systemic Venous pressure in Fontan Some degree of congestion (Venous pressure >/= PAP) Little variability at rest from 13 to 20 mm Hg Mildly increased at exercise. Pressures above 20 mmHg are rarely seen Determinants of Left Atrial Pressure AV Valve Diastolic Function AV synchrony Fenestration Marc Gewillig et al. Interactive CardioVascular and Thoracic Surgery 10 (2010) 428–433
- 24. Transpulmonary Resistance • Fontan Connection Resistance • Gradient across fontan circuit poorly tolerated Dec CO • Causes: • Stenosis • Resistance offered by :- valves , conduits ,patches • Flow dynamics and flow resistance Laminarity of flow Type of anastamosis Marc Gewillig et al. Interactive CardioVascular and Thoracic Surgery 10 (2010) 428–433
- 25. Pulmonary Vascular Resistance • Major determinant of cardiac output • Drugs decreasing PVR improves cardiac output • Baseline PVR predicts future outcomes
- 26. Worsening PVR Subotpimal PA growth Absence of Pulsatile pulmonary flow Functional Loss of Lung segments with ageing Pulmonary lymphatic edema Chronic use of Amiodarone Living at High altitiude Kreutzer et al Frontiers in Paediatrics December 2013
- 27. Evolution of Fontan concept
- 28. Atriopulmonary Fontan and Kreutzer • First Generation (1971) Lateral Tunnel Fontan • Second Generation (1987) The Extracardiac Conduit Fontan Procedure • Third Generation (1990) Intra/Extracardiac Conduit With Fenestration • Fourth generation (1987)
- 32. Advantage Conduit enlarges as the child grows - may be used in children as young as 1 year old Decreased blood stasis and risk of thrombosis Limited portion of RA exposed to high venous pressures (reduces risk of arrhythmias) Coronary sinus remains in low pressure atrium (allows unimpended myocardial venous drainage)
- 35. • Advantages : – No or minimal CPB – Entire atrium is left with low pressure - less atrial distention, arrhythmia, and thrombosis. – Avoids RA incisions and extensive atrial sutures – Reduces risk of sinus node injury – Reduces incidence of post op arrhythmias • Disadvantages : – Cannot enlarge as the child grows – Performed only in child large enough to accept a graft of adequate size to allow adult IVC blood flow. – Risk of obstruction by thrombus formation or neo intimal hyperplasia
- 36. Comparison Atrio-pulmonary Lateral tunnel Extra cardiac Growth + + - Surgical procedure Open cardiac Open cardiac Closed Atrial suture + ++ - Atrial dilation/ arrhythmias ++ + +/- SA nodal dysfunction + + - Thrombus formation ++ - + Laminar flow - + +
- 37. Fenestrated Fontan • small opening or fenestration may be created between the conduit and the right atrium • Functions as a pop-off valve (a right-to-left shunt) – prevent rapid volume overload to the lungs – Limit caval pressure – Increase preload to the systemic ventricle – Increase cardiac output • cyanosis may result from the right-to-left shunt
- 39. Harms Benefits Source of Qs, bypassing PVR Increases preload > CO Limits or decrease CVP rise acutely Desaturation Paradoxical Embolization Need to close later
- 40. • Fenestration was performed selectively in 32 patients (39%), including only 2 of the last 38 (5%). • Prolonged (> 2 weeks) pleural drainage occurred in 13 patients, 8 with fenestration and 5 without. • Fenestration is not necessary in most Fontan patients when an extracardiac conduit technique is performed • Should not be performed routinely • Need for fenestration should be assessed after cardiopulmonary bypass when hemodynamics can be evaluated accurately.
- 41. Fenestrate or Not ? • Currently fenestration only in “high-risk” patients • High PVR (>2 U/m2) or high mean PA pressure (>18 mm Hg) • Distorted PAs secondary to previous shunt operations • Poor systolic or diastolic ventricular function, with LV end-diastolic pressure greater than 12 mm Hg or an ejection fraction less than 60% • AV valve regurgitation Lateral tunnel fontan Fenestratiom size <12kg 4mm 12-30kg 5mm >30kg 6mm
- 42. Whether and when to close ? • Most of them close gradually and spontaneously (40 % 1) • Delayed closure • Benefits of increasing saturation translating in favorable outcomes for body growth • Optimal timing is unknown2 • Indication2 • Aortic saturation <90% • Tolerance of BALLOON occlusion test
- 43. Procedure • Evaluate arterial and venous collaterals • About 15 to 20 min after the balloon occlusion, changes of pressure and saturation within the Fontan circuit, left atrium and aorta. Criteria for fenestration closure is : 1. Right atrial pressure (Fontan Circuit) ≤ 18 mmHg 2. Increase in the difference of arteriovenous oxygen saturation ≤ 33%, 3. Right atrial saturation (Fontan Circuit) ≥ 40% 4. < 30 % drop in Qs 5. Increase in the mean RA pressure <4 mmHg
- 44. Intra-Extra Cardiac conduit with Fenestration the internal orifice of the inferior vena cava
- 45. Intra-Extra Cardiac conduit with Fenestration
- 47. How to achieve a Fontan Circuit At BIRTH, it is impossible to create a Fontan circulation: PVR is elevated for several weeks SVC and IVC veins and pulmonary arteries may be too small STAGED APPROACH Adapt to changing hemodynamics
- 48. How to achieve a Fontan Circuit Neonatal period (1 month) Improve the limited flow to the lungs – BT SHUNT / PA BAND The infant is allowed to grow for several months Pulmonary vasculature will develop more PVR will stabilize PROBLEMS The heart will be subjected to chronic volume overload / pressure overload Ventricular function may deteriorate Expect mild progressive desaturation of the infant
- 49. How to achieve a Fontan Circuit At age 4-12 months The superior vena cava will be connected to the pulmonary artery (Glenn) This will decrease the volume load to the heart The patient will remain cyanotic as the desaturated blood from the IVC is still allowed to flow to the aorta
- 50. How to achieve a Fontan Circuit At 1-5 years of age The Fontan circuit is completed by connecting the IVC to the pulmonary artery Single Ventricle – Bidirectional Glenn Single Ventricle – Completed Fontan http://www.cincinnatichildrens.org/health/heart-encyclopedia/anomalies/sv.htm
- 51. FONTANS STAGING SUMMARY STAGE 1: AT 1 MONTH OF AGE OPTIMISE QP/QS : BT SHUNT / PA BAND STAGE 2: AT 4-12 MONTHS OPTIMISE VENTRICULAR VOLUME: BD GLENN / HEMI FONTAN STAGE 3: AT 1-5 YEARS REDUCE ADMIXTURE & DIRECT FUNCTIONAL VENTRICLE TO SYSTEMIC CIRCUIT FONTANS
- 52. Fontan FAILURE Fontan failure is defined as: NYHA functional class III or IV Death Fontan Take-down / Conversion Cardiac Transplantation
- 53. FONTAN COMPLICATIONS ANATOMIC LOCATION COMPLICATION Left ventricle Ventricular failure causing exercise intolerance,ischemia and infarction Pulmonary circulation Stenosis,dilatation or leakage of anastomosis;pulmonary artery stenosis ;pulmonary hypertension IVC Increased pressures causing cirrhosis,liver failure and portal hypertension;increased risk for liver carcinoma RA with classic fontan circulation Dilatation(can be severe);poor turbulent flow;blood clot formation Collateral vessels and shunts Pulmonary AVM,aortopulmonary collateral vessels Lymphatic system Protein losing enteropathy,plastic bronchitis, pericardial and pleural effussion,chylothorax Blood vessels Clot,emboli including pulmonary embolism
- 56. Arrhythmias • includes sinus node dysfunction, predominant junctional rhythm, atrioventricular block, supraventricular and ventricular arrhyth- mias, and the risk of arrhythmic sudden death. • Sinus node dysfunction is reported in • 40% of patients with atriopulmonary connections, • 25% of lateral tunnel and extracardiac cavo- pulmonary connection surgeries
- 58. • Risk factors for the development of atrial tachycardia include an 1. atriopulmonary connection, 2. preoperative bradycardia, 3. lack of sinus rhythm, 4. older age at Fontan and longer postoperative interval, 5. greater than mild atrioventricular valve regurgitation, 6. heterotaxy syndrome.
- 59. • Atrial reentrant tachycardia accounts for approximately 75% of supraventricular tachycardia, with focal atrial tachycardia in up to 15% of patients. • In lateral tunnel patients, the reentrant circuit may reside in the pulmonary venous atrium. • Atrial fibrillation is becoming increasingly common in adult Fontan patients, and is present in almost half of patients referred for Fontan conversion.
- 61. • Acute success rates from catheter ablation in the Fontan patient range from 40-75%, with recurrence of tachycardia in 60% of patients during the first year. • best suited for patients with lateral tunnel repairs and focal atrial tachycardia, or atriopulmonary repairs who are not suitable candidates for Fontan arrhythmia surgery. within 24e48 h from onset lower success rates
- 63. • Extra cardiac Conduit – IVC to PA • Bidirectional Glenns Shunt – SVC to PA • Resection of the diated Right Atrium • Maze Procedure (Anti-arrythmic) • Epicardial Pacemaker Fontan Conversion
- 64. Fontans Complications LYMPHATIC SYSTEM High venous pressure & impaired thoracic duct drainage Lymphatic system dysfunction. Increased pulmonary lymphatic pressure interstitial pulmonary edema or lymphedema. Leakage into the thorax or pericardium PERICARDIAL AND PLEURAL EFFUSIONS (often right-sided) and CHYLOTHORAX Rx – Reduce CVP , Fenestration , Fontan Conversion / Take down
- 65. • Fu et al compared patients who underwent extracardiac conduit Fontan procedure with and without a fenestration. • The duration of pleural drainage with a fenestration was 10 days ± 12 days, while without a fenestration the duration was 13.2 days ± 8.8 days (P .016). Pleural effusion
- 66. Fontans Complications LYMPHATIC SYSTEM PROTEIN-LOSING ENTEROPATHY (5-15%%) Time of presentaion - weeks to years after Fontan, mean ≈ 3.5 years Its cause is unclear Elevated systemic venous pressure Elevated hepatic and portal venous pressure Loss of enteric protein Interstinal Lymphangiectasis Loss of enteric protein Hypoproteinemia, Immunodeficiency, Hypocalcemia, And Coagulopathy Fatigue, Peripheral Edema, Pleural & Pericardial Effusions,weight loss, Ascites,lalabsorption & Chronic Diarrhea. Low serum albumin level & Increased fecal α1- antitrypsin levels
- 67. PLE 50% mortality at 5 yrs Time from PLE Diagnosis Recent data from some centers show with treatment advances, survival has improved to 88% and 72% after diagnosis at 5 and 10 years, respectively.
- 68. Treatment Hemodynamic stabilization Hemodynamic stabilization Decompress atrium( fenestration) Improve hemodynamics – vasodilators Nutritional stabilization Diet : Calories dense, high protein, rich in MCT, salt restricted Maintain protein : Albumin +/- globulin infusion regularly Supportive measures to avoid infections – antibiotic Px, vaccines Judicious diuretic use, Fenestration / Fontan Conversion / Cardiac Transplantation
- 69. Plastic Bronchitis • Rare condition , Incidence 3- 4% • Risk Factors – Same as PLE • Formation of mucofibrinous bronchial casts resulting in marked airway obstruction. • Patients will often expectorate these casts or require removal by bronchoscopy • Life-threatening events may occur in up to 40 percent of affected patients • Management – Same as PLE • Proposed treatment options • Inhaled or systemic steroid • Aerosolized mucolytics • Aerosolized fibrinolytics such as tissue plasminogen activator
- 70. Fontan Circulation Complications BLOOD VESSELS Predisposition to COAGULOPATHIES Thrombosis is more likely in patients with low CO and venous stasis Increased incidence of coagulation factor abnormalities because of Hepatic Congestion Protein C Protein S ATIII deficiency Chronic cyanosis–induced Polycythemia Leads to chronic / recurrent Pulmonary Embolism Anticoagulation / Asprin Prophylaxis of all patients is controversial
- 72. Thromboembolism • Incidence varies from 6% to 25%. • Bimodal Peak • Risk Factor • Supraventricular arrhythmias • Right atrial dilation • Artificial material used to construct the Fontan circuit • Right atrial “smoke” • Fenestrated Fontan circuit • Protein C deficiency
- 73. • N = 111 • 2 years either ASA (5 mg/kg/day, no heparin phase) or warfarin (started within 24 h of heparin lead-in; INR : 2.0 to 3.0) • Overall freedom from thrombosis 2 years after Fontan surgery was 19%, despite thrombosis prophylaxis • 86 % ECTC , 60 % fenestrated • No significant difference between ASA and heparin/warfarin as primary thromboprophylaxis
- 74. Annual Follow up Monitoring Constitutional Symptoms Aerobic activity, Exercise Testing Cardiac Hemodynamics CXR / ECHO / CT or MRI Rhythm ECG/Holter Pulmonary Saturation resting / Exertional Hepatic LFT / USG liver Gastrointestinal Stool alpha 1 anti-trypsin
- 75. CARDIAC TRANSPLANTATION • Failing Fontan circulation can benefit from orthotopic cardiac transplantation. • The main indications for transplantation: – Heart failure – Intractable arrhythmias – Protein-losing enteropathy – Plastic bronchitis
- 77. SEQUELAE OF FONTAN OPERATION • Perioperative mortality : 3-5 % (< 2 % in recent data) • Overall survival – 5 yrs – 86% – 10 yrs – 81% – 15 yrs – 73% • 10 yr survival (lateral tunnel) – 87% • 10 yr survival (extracardiac) – 92.4%
- 78. • Independent predictors of mortality: 1. Pre-op high PA pressure 2. Severe infection in early post-op period 3. Early morbidities : 4. Pleural and pericardial effusion 5. Low cardiac output 6. Sinus node injury 7. Pulmonary and systemic venous obstruction
- 79. • Factors asso. with long term morbidity: 1. Progressive ventricular dysfunction 2. Systemic venous hypertension 3. RA distension (classical) 4. Thromboembolic episodes 5. Worsening cyanosis 6. Heterotaxy syndromes 7. Significant AV valve regurgitation 8. NYHA class III / IV (pre-op) 9. Elevated PA pressure (pre-op)
- 80. Survival Improvement in Surgical Results over time frames 5 Year survival 78.5% 10 Year survival 71.4% Gentles et al JTCVS 1997 Postoperative 15- to 20-year survival rates after Fontan procedure range from 60 to 85 percent
- 81. Survival has improved ! Yves d’Udekem et al Circulation 2007 Hospital Survivors 10-year survival 91 % 20-year survival 84 % 94 % 81 %
- 82. Kreutzer GO. Thirty-two years after total right heart bypass. J Thorac Cardiovasc Surg 2007 Longest lived patient, 39 yrs after surgery, 8 years after conversion Current age 57 years
- 83. Conclusion • Offers only definitive surgical palliation for wide variety of complex CHD with single dominant ventricle • Fifth Decade Now , quest for Ideal fontan Continues • Perioperative and early mortality has decreased markedly over the past 4 decades. • ICEC Fenestrated Fontan had shown early promising results • Routine Fenestration and Anticoagulation is controversial • Identification of ‘failing’ Fontan before development of complications is essential to improve outcomes. • Fontan Conversion remains hope for older fontan patients IT’S DEFENITELY NOT THE END OF THE ROAD MUCH HAS BEEN ACHIEVED, AND MORE HAS TO COME!
- 84. Recent Advances
- 85. Fontan completion without surgery Fontan preparation
- 86. • 34 patients underwent Fontan preparation with BDCPC. • Median age was 7.7 months (5 to 51) • Median intensive care and hospital stay durations were 1 and 6 days • None of the patients required inotropes, chest tube insertion, or mechanical ventilation. • Overall survival after BDCPC with Fontan preparation was 77%. • Despite longer bypass and ischemic times, Fontan preparation at time of BDCPC was feasible • Excellent early dynamics, and echocardiographic and clinical outcomes Ann Thorac Surg 2011;91:566–73
- 87. Percutaneous insertion Reversal of Fontan Paradox Normalization of hemodynamics J Thorac Cardiovasc Surg. 2013 January
- 88. “Those who believe that one ventricle can drive blood full of spirit into the body and the lungs likewise, are heretics. They forget that nature, being divine, never gave a heart to any where there was no need ” William Harvey
- 89. Thank You