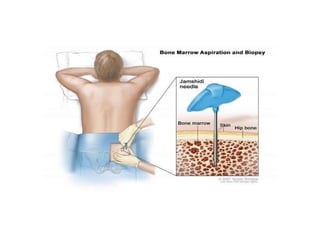
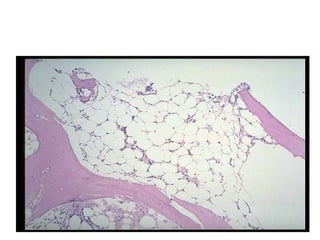
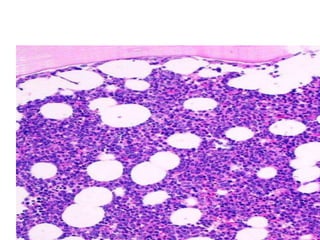
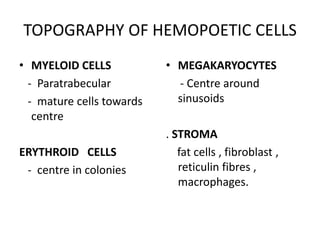
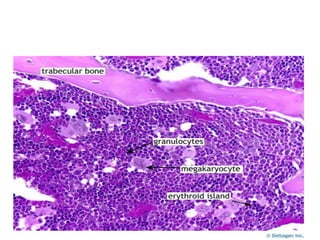
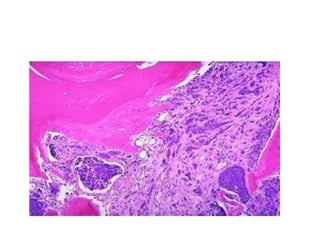
The document discusses bone marrow biopsy techniques and evaluation. It describes the structure of bone marrow, including cellular elements and stroma. Needle types and biopsy sites are covered. Processing involves fixation, decalcification, embedding and staining. Evaluation is based on clinical history, hemogram, smear and aspiration. Adequacy, cellularity, cell topography, proliferation, fibrosis, infections, and infiltrative diseases are assessed. Stromal changes like fibrosis and necrosis are also evaluated. Common conditions affecting bone marrow including CML, MDS, Hodgkin's, NHL, CLL and metastasis are discussed. Adequate history, processing, cellularity, topography, stromal changes, infections and gran