Downloaded 11 times

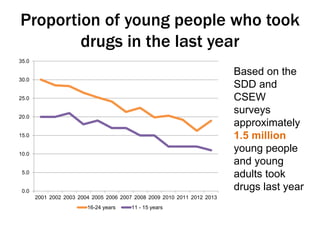
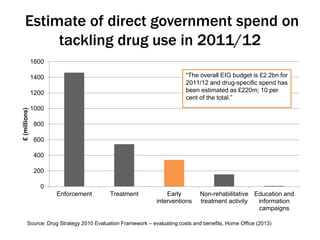
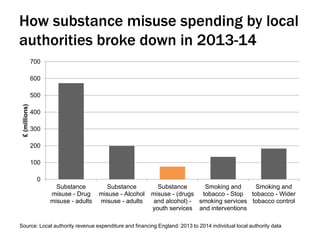
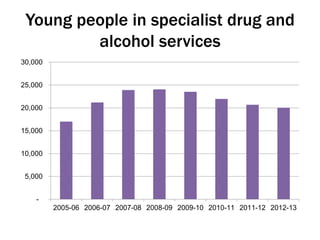
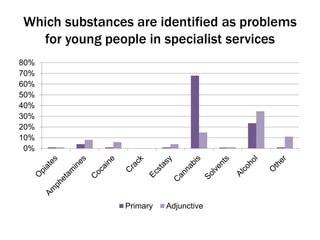
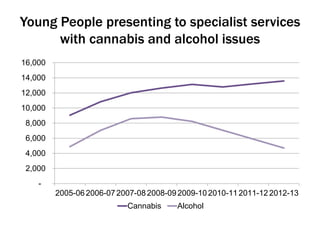
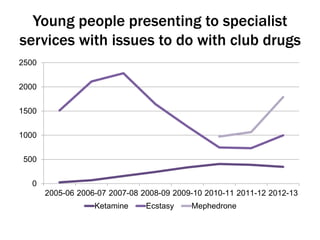
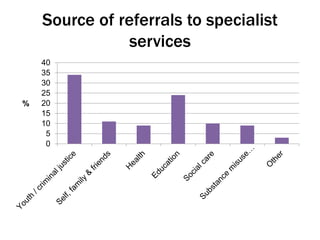


The document discusses the context and challenges of substance use among young people, noting that while most do not use drugs regularly, a subset requires specialized treatment which incurs significant costs. It highlights the shift in responsibility for drug policy from the Department for Education to the Home Office and Department of Health, and the impact of funding cuts on services for young people. Additionally, the document emphasizes the need for integrated strategies to address substance misuse and the importance of tailored interventions for at-risk youth.








![Ecosystems of prevention: building local practice networks [EUSPR 2016]](https://cdn.slidesharecdn.com/ss_thumbnails/euspr2016-161108105905-thumbnail.jpg?width=640&height=640&fit=bounds)







































![Smoking, drinking and drug use by young people in England [2017 update]](https://cdn.slidesharecdn.com/ss_thumbnails/adepisppstatsupdate14-170418123929-thumbnail.jpg?width=640&height=640&fit=bounds)



















































