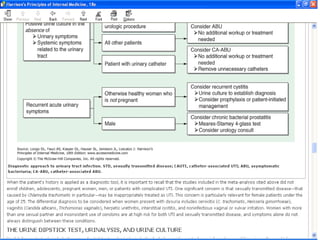
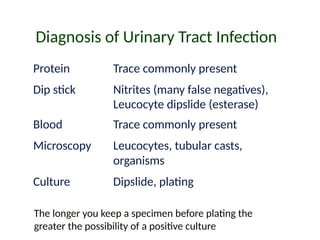
The document provides a comprehensive overview of urinary tract infections (UTIs), including their definitions, epidemiology, risk factors, etiology, pathogenesis, diagnosis, treatment, and prognosis. It emphasizes the distinction between uncomplicated and complicated UTIs, highlighting diagnostic approaches and treatment strategies for various patient demographics, including pregnant women and men. Key factors such as the prevalence of E. coli as a causing agent and risk factors like gender and sexual behavior are also discussed.






















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














