User Centered Design and Rapid Prototyping supported by a Wiki to develop a Decision Aid for CPR and Mechanical Ventilation adapted to the Context of an Intensive Care Unit
•
1 like•287 views

Poster with preliminary results for www.wikidecision.org project http://www.researchprotocols.org/2016/1/e24/

More Related Content
What's hot
What's hot (18)
Similar to User Centered Design and Rapid Prototyping supported by a Wiki to develop a Decision Aid for CPR and Mechanical Ventilation adapted to the Context of an Intensive Care Unit
Similar to User Centered Design and Rapid Prototyping supported by a Wiki to develop a Decision Aid for CPR and Mechanical Ventilation adapted to the Context of an Intensive Care Unit (20)
More from Patrick Archambault
More from Patrick Archambault (13)
Recently uploaded
Recently uploaded (20)
User Centered Design and Rapid Prototyping supported by a Wiki to develop a Decision Aid for CPR and Mechanical Ventilation adapted to the Context of an Intensive Care Unit
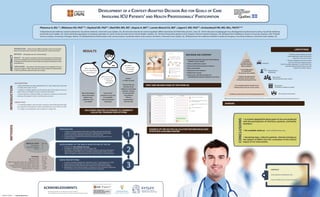
- 1. Plaisance A, BSc1,2 ; Witteman HO, PhD3,4,9 ; Heyland DK, PhD5,6 ; Ebell MH, MD, MS7 ; Dupuis A, MA2,8 ; Lavoie-Bérard CA, MD2 ; Légaré F, MD, PhD4,9 ; Archambault PM, MD, MSc, FRCPC2,4,9 1 Département de médecine sociale et préventive, Faculté de médecine, Université Laval, Québec, QC ; 2 Centre de recherche du Centre hospitalier affilié universitaire de l’Hôtel-Dieu de Lévis, Lévis, QC ; 3 Vice-décanat à la pédagogie et au développement professionnel continu, Faculté de médecine, Université Laval, Québec, QC ; 4 Axe Santé des populations et pratiques optimales en santé, Centre de recherche du CHU de Québec, Québec, QC ; 5 Clinical Evaluation Research Unit, Kingston General Hospital, Kingston, ON ; 6 Department of Medicine, Queen’s University, Kingston, ON ; 7 Health Sciences Campus, University of Georgia, Athens, GA ; 8 Département d’information et de communication, Faculté des lettres et des sciences humaines, Université Laval, Québec, QC ; 9 Département de médecine familiale et médecine d’urgence, Faculté de médecine, Université Laval, Québec, QC. DEVELOPMENT OF A CONTEXT-ADAPTED DECISION AID FOR GOALS OF CARE INVOLVING ICU PATIENTS' AND HEALTH PROFESSIONALS' PARTICIPATION INTRODUCTION Intensivists face difficult situations which raise questions about the informed nature of decision making about life-sustaining therapies. METHODS Ethnography and user-centered design. RESULTS We created a novel paper and wiki-based decision aid (DA) about goals of care adapted to the needs of a local ICU. We identified multi-level barriers to making end-of-life decisions in the ICU that are congruent with patients’ values and preferences. CONCLUSIONS We produced a DA about goals of care adapted to the local context of a single ICU. Many steps still need to be done before its implementation in this ICU and before scale-up to other care settings. ABSTRACT BACKGROUND • Many frail elderly are being admitted to ICUs. Upon admission, they need to clarify their goals of care. • Inability to engage patients in discussions about their goals of care can lead to the use of aggressive life-sustaining therapies. • Shared decision-making (SDM) can improve congruence of decision making with patients’ values and decreases overuse. OBJECTIVES • To identify patients’ and clinicians’ needs for end-of-life decisions that are congruent with patients’ values and preferences (e.g. CPR or no CPR) • To adapt an existing DA to the context of a single ICU. INTRODUCTIONMETHODS ACKNOWLEDGMENTS We thank all participants, including the critically-ill patients who contributed to improving our decision aid for the benefit of future patients. RESULTS • A context-adapted DA about goals of care was produced with the participation of clinicians, patients, and family members. • DA available online at www.wikidecision.org • Upcoming steps : video for patients, clinician training on the subject of SDM in the ICU, evaluation of the clinical impact of our intervention. CONCLUSIONS PREPARATION • 3 weeks of ethnographic information of daily interactions between patients, families, intensivists and other allied health professionals • 4 semi-structured individual interviews with intensivists • 5 observations of patient-intensivist discussions about goals of care • Content analysis 1 2 3 DEVELOPMENT OF THE WIKI & ADAPTATION OF THE DA • Creation of www.wikidecision.org • Translation and adaptation of a DA about CPR • Translation and integration of the Good Outcome Following Attempted Resuscitation (GO FAR) score to predict neurologically intact survival after in-hospital cardiopulmonary resuscitation into the wiki-based DA RAPID PROTOTYPING • 3 cycles of rapid prototyping (5 dyads by cycle, 15 participants in total) • Observations of prototype use with a structured observation grid • Short interviews with patients and intensivists and content analysis • Modification of the DA prototype in response to the comments addressed prior to the next cycle in each iteration of the prototype MEDICAL STAFF Intensivists Medical residents Nurses N = 10 6 2 2 PATIENTS Age mean (SD) Women, N (%) High school education not completed, N (%) Medical reason for admission, N (%) Length of stay in the ICU (days), mean (SD) Catholic faith (practicing or not), N (%) Mortality post-3 months N = 15 67 (16) 8 (53) 4 (27) 13 (87) 5 (3) 12 (80) 3 (20) More information about alternative options (e.g. palliative care) was added Focus of the questions on current & acceptable future functional autonomy It does ! in 100% of cases The GO FAR rule and Icon Array software to illustrate patients’ chances of survival with and without CPR was programmed into the wiki What will happen to me if I refuse those interventions ? What are the risk to loose my functional autonomy ? Untreated cardiac arrest can not lead to death... SOLUTIONS CREATED ACCORDING TO COMMENTS COLLECTED THROUGH PROTOTYPING FIRST AND SECOND PAGES OF THE PAPER DA DECISION AID CONTENT • International Patient Decision Aid Standards (IPDAS) criteria (20/30) • Values clarification section • General information about procedures • Risks and benefits • Population-level statistics • Deliberation section • Online only : GO FAR calculator for individualized statistics linked to Icon Array Cet outil a été produit grâce à la collaboration de ... et de patients admis à l’Unité des soins intensifs de l’Hôtel-Dieu de Lévis et de leurs proches. Dernière mise à jour le 20 mai 2016 Outil d’aide à la décision sur les objectifs de soins Version destinée aux patients aptes admis à l’unité des soins intensifs de l’Hôtel-Dieu de Lévis Introduction Lors d’une hospitalisation, l’équipe soi- gnante discutera avec vous et vos proches corresponde à vos objectifs de soins. Il sera plus particulièrement question de vos valeurs et de votre niveau d’autonomie actuel et de deux interventions : la réanimation cardiorespiratoire (RCR) la ventilation mécanique Ce document a été conçu pour vous aider à prendre une décision éclairée à ce sujet. 2 Que se passera-t-il après que j’ai discuté de mes objectifs de soins ? Vos objectifs de soins seront inscrits à votre dossier et votre plan de traitement sera ajusté en conséquence. Si vous changez d’idée, faites-le savoir à un membre de l’équipe. Si vous avez des questions ou des pré- occupations à propos de l’information fournie dans cette brochure, sentez-vous à l’aise d’en discuter avec l’équipe soignante. 11 SURVIE À TOUT PRIX CONFORT Prolonger la vie par tous les soins nécessaires Prolonger la vie par des soins limités Assurer le confort prioritairement à prolonger la vie Assurer le confort uniquement sans viser à prolonger la vie BARRIERS Multi-level barriers leading to an end-of-life in the ICU that is incongruent with patients’ values and preferences Individual Patient/Doctor relationhsip Microsystem (clinical practices, team culture) Mesosystem (institutions, healthcare system) Macrosystem (community) • Lack of knowledge of intensive care and interventions that are offered • Lack of data about our population • No decision aid available • Patients transferred from the ED to the ICU without having discussed goals of care • No centralized patient health record • Medical doctor fee-per-service system • Healthcare system bias towards keeping people alive • The DA could not address all needs (video explanation, better information about how non-survivors die) • The DA is adapted to the local context of an ICU serving an aging Caucasian French Canadian population. It would need to be culturally adapted before being used with patients from other cultures. LIMITATIONS EXAMPLE OF THE GO FAR CALCULATOR FOR INDIVIDUALIZED STATISTICS AVAILABLE ONLINE ImagescreatedbyIconarray.com www.wikidecision.org/comments arianeplaisance@gmail.com CONTACT GRAPHIC DESIGN | depicsci@gmail.com