Adaptation of DECISION+: a Training Program in Shared Decision Making on the Use of Antibiotics for Acute Respiratory Infections in Primary Care to the Context of an Emergency Department - a Mixed Methods Study
•
1 like•530 views

Poster presented at the 2016 Canadian Association of Emergency Physicians conference about the adaptation of the Decision+ program about using antibiotics for upper respiratory infections developed in primary care for the context of Emergency Medicine
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Adaptation of DECISION+: a Training Program in Shared Decision Making on the Use of Antibiotics for Acute Respiratory Infections in Primary Care to the Context of an Emergency Department - a Mixed Methods Study
Similar to Adaptation of DECISION+: a Training Program in Shared Decision Making on the Use of Antibiotics for Acute Respiratory Infections in Primary Care to the Context of an Emergency Department - a Mixed Methods Study (20)
More from Patrick Archambault
More from Patrick Archambault (13)
Recently uploaded
Recently uploaded (20)
Adaptation of DECISION+: a Training Program in Shared Decision Making on the Use of Antibiotics for Acute Respiratory Infections in Primary Care to the Context of an Emergency Department - a Mixed Methods Study
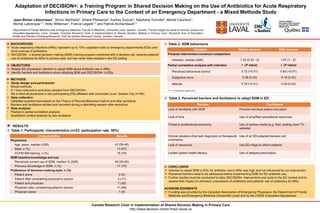
- 1. Adaptation of DECISION+: a Training Program in Shared Decision Making on the Use of Antibiotics for Acute Respiratory Infections in Primary Care to the Context of an Emergency Department - a Mixed Methods Study Jean-Simon Létourneau1, Simon Berthelot1, Ariane Plaisance2, Audrey Dupuis2, Stéphane Turcotte3, Michel Cauchon1, Michel Labrecque1,3, Holly Witteman1, France Légaré1,3 and Patrick Archambault1,2 1Department of Family Medicine and Emergency Medicine, Faculty of Medicine, Université Laval, Quebec, Canada; 2Centre intégré de santé et services sociaux de Chaudière-Appalaches, Lévis, Canada; 3Canada Research Chair in Implementation of Shared Decision Making in Primary Care, Research Axis of Population Health and Practice-Changing Research, CHU de Québec Research Centre, Quebec, Canada ► BACKGROUND v Acute respiratory infections (ARIs) represent up to 10% outpatient visits to emergency departments (EDs) and drive overuse of antibiotics. v DECISION+, a shared decision making (SDM) training program combined with a decision aid, reduces patients' use of antibiotics for ARIs in primary care, but has never been studied in the ED setting. ► METHODS v Study design and participants: • Mixed-methods • A 1-hour interactive workshop adapted from DECISION+. • We invited all physicians in two participating EDs affiliated with Université Laval, Quebec City (n=56). v Data collection: • Validated questionnaire based on the Theory of Planned Behaviour before and after workshop. • Barriers and facilitators elicited and recorded during a debriefing session after workshop. v Data analysis: • Pearson’s partial correlation analysis • Qualitative content analysis by two reviewers ► CONCLUSION v Intention to adopt SDM in EDs for antibiotic use in ARIs was high and not influenced by our intervention. v Perceived barriers need to be addressed before implementing SDM for ED antibiotic use. v Further studies must be conducted to tailor DECISION+ interventions and tools to the ED context and to assess their impact on clinicians’ prescription of antibiotics and patients’ use of antibiotics for ARIs. ACKNOWLEDGMENTS v Funding was provided by the Canadian Association of Emergency Physicians, the Department of Family Medicine and Emergency Medicine (Université Laval) and by the CISSS Chaudière-Appalaches. Canada Research Chair in Implementation of Shared Decision Making in Primary Care http://www.decision.chaire.fmed.ulaval.ca ► RESULTS v Table 1. Participants’ characteristics (n=23; participation rate: 50%) v Table 3. Perceived barriers and facilitators to adopt SDM in ED ► OBJECTIVES v Assess ED physicians’ intention to adopt SDM about antibiotic use in ARIs. v Identify barriers and facilitators about adopting SDM and DECISION+ in EDs. Characteristics Results Physicians Age, years, median (IQR) 42 (36-48) Male, n (%) 13 (57) CCFM-EM training, n (%) 18 (78) SDM baseline knowledge and use Perceived current use of SDM, median % (IQR) 40 (20-50) Previous knowledge of SDM, n (%) 17 (74) Preference of decision-making style, n (%) Patient alone 0 (0) Patient after considering physician's opinion 4 (17) Patient and physician 7 (30) Physician after considering patient's opinion 11 (48) Physician alone 1 (4) v Table 2. SDM behaviours * P = 0.15 (Wilcoxon signed-rank) Variables Before seminar After seminar Pre/post intervention construct comparison Intention, median (IQR) 1.33 (0.33 - 2) 1.67 (1 - 2)* Partial correlation analysis with intention r (P value) r (P value) Perceived behavioral control 0.72 (<0.01) 0.60 (<0.01) Subjective norm 0.28 (0.23) 0.18 (0.42) Attitude 0.76 (<0.01) 0.29 (0.20) Barriers Facilitators Lack of familiarity with SDM Provide individual patient education Lack of time Use of simplified educational resources Threat to professional autonomy Use of various media (e.g. flyer, waiting room TV, website) Clinical situations that lack diagnostic or therapeutic uncertainty Use of an ED-adapted decision aid Lack of resources Use ED triage to inform patients Limited patient health literacy Use of delayed prescription