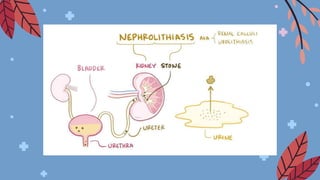
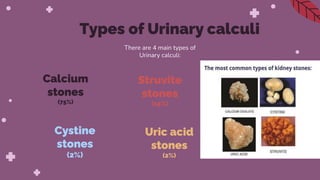
Nephrolithiasis refers to kidney stones formed within the kidneys or other parts of the urinary tract. There are four main types of stones: calcium stones, which are the most common; struvite stones, which can form due to urinary tract infections; uric acid stones, associated with high protein diets and gout; and cystine stones, caused by a hereditary condition. Stones may cause complications if they block the urinary tract, including infection, kidney damage, and renal failure. Treatment depends on the size and location of the stone and may include pain medications, increased fluids, surgery to break up or remove stones.