Steps in ascendinginfection
1st colonization of distal urethra and introitus (in the
female) by bacteria
From urethra to the bladder (by catheterization or
instrumentation) or in females due to short urethra,
no anti-bacterial prostatic fluid, hormonal changes
affecting adherence of bacteria to the mucosa, sex-
related urethral trauma
Multiplication of bacteria in the bladder (favored by
outflow obstructon)
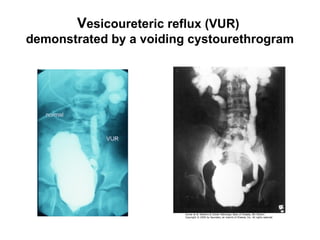
Vesicoureteric reflux through incompetent
vesicoureteral orifice
Intrarenal reflux through open papillae to kidney
6.
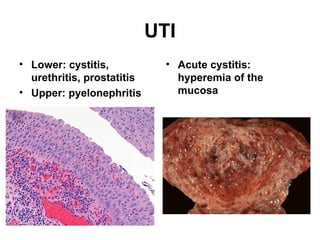
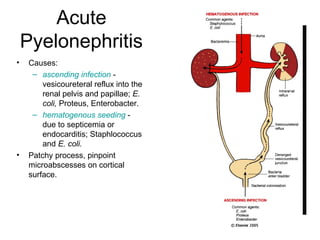
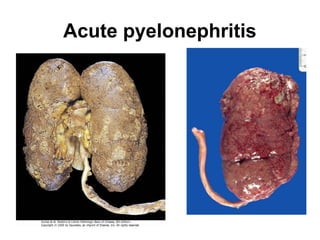
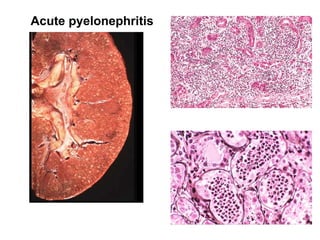
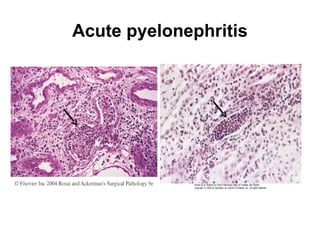
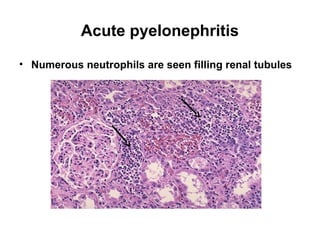
Acute
Pyelonephritis
• Causes:
– ascendinginfection -
vesicoureteral reflux into the
renal pelvis and papillae; E.
coli, Proteus, Enterobacter.
– hematogenous seeding -
due to septicemia or
endocarditis; Staphlococcus
and E. coli.
• Patchy process, pinpoint
microabscesses on cortical
surface.
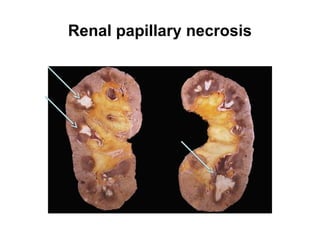
Complications of acutepyelonephritis
• Papillary necrosis: coagulative necrosis of
tubules; common in DM & urinary tract
obstruction, usually bilateral
• Perinephric abscess: extension of pus into
adjacent tissue
• Pyonephrosis (pelvis filled with pus): total or
almost complete obstruction prevents
drainage of pus
• Chronic pyelonephritis
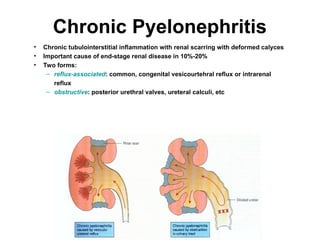
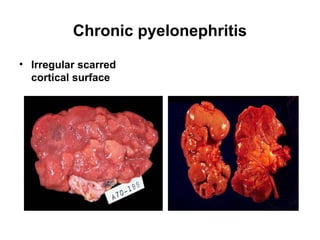
Chronic Pyelonephritis
• Chronictubulointerstitial inflammation with renal scarring with deformed calyces
• Important cause of end-stage renal disease in 10%-20%
• Two forms:
– reflux-associated: common, congenital vesicourtehral reflux or intrarenal
reflux
– obstructive: posterior urethral valves, ureteral calculi, etc
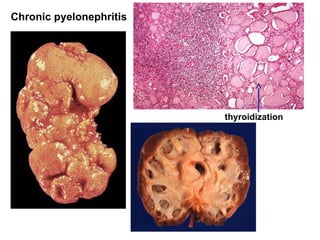
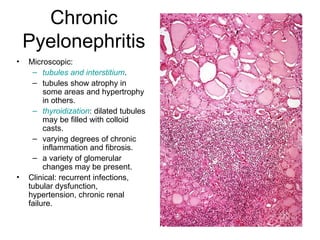
Chronic
Pyelonephritis
• Microscopic:
– tubulesand interstitium.
– tubules show atrophy in
some areas and hypertrophy
in others.
– thyroidization: dilated tubules
may be filled with colloid
casts.
– varying degrees of chronic
inflammation and fibrosis.
– a variety of glomerular
changes may be present.
• Clinical: recurrent infections,
tubular dysfunction,
hypertension, chronic renal
failure.
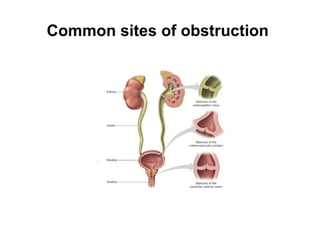
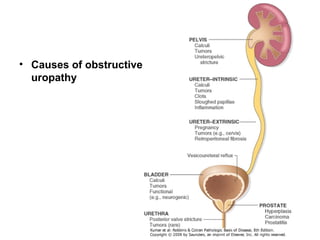
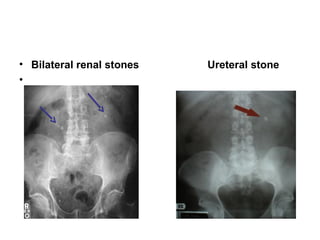
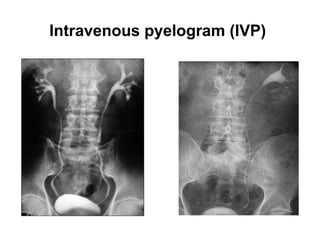
Obstructive uropathy
o Unilateralor bilateral
o From urethra to renal pelvis
o ↑ susceptibility to infection & stone
formation
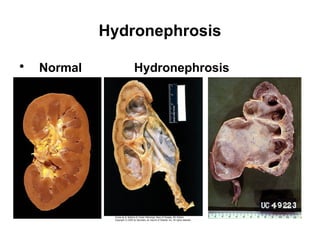
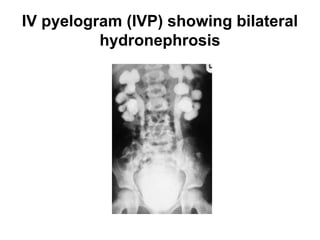
o Chronic obstruction causes hydronephrosis:
cystic pelvis & calyceal dilation with
progressive cortical atrophy
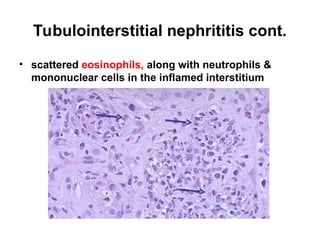
Tubulo-interstitial disorders
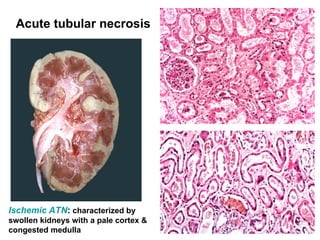
Acute tubularnecrosis
• Acute renal failure associated with dysfunction & necrosis of tubular
epithelial cells
• Classification:
– ischemic: shock, sepsis, burns, transfusion, other
– toxic: drugs, metals, poisons, solvents, other
• focal to extensive epithelial necrosis
• Pathogenesis:
– vasoconstriction, obstruction, tubular leakage of filtrate.
Oliguric phase (risk of hyperkalemia) => diuretic phase (risk of
hypokalemia)
Prognosis depends in part on the cause
31.
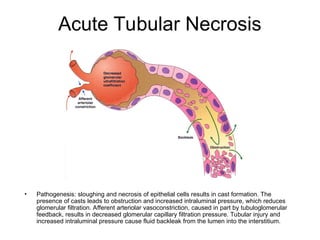
Acute Tubular Necrosis
•Pathogenesis: sloughing and necrosis of epithelial cells results in cast formation. The
presence of casts leads to obstruction and increased intraluminal pressure, which reduces
glomerular filtration. Afferent arteriolar vasoconstriction, caused in part by tubuloglomerular
feedback, results in decreased glomerular capillary filtration pressure. Tubular injury and
increased intraluminal pressure cause fluid backleak from the lumen into the interstitium.
32.
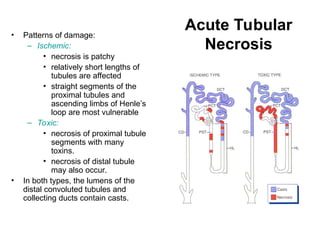
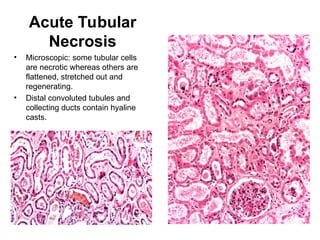
Acute Tubular
Necrosis
• Patternsof damage:
– Ischemic:
• necrosis is patchy
• relatively short lengths of
tubules are affected
• straight segments of the
proximal tubules and
ascending limbs of Henle’s
loop are most vulnerable
– Toxic:
• necrosis of proximal tubule
segments with many
toxins.
• necrosis of distal tubule
may also occur.
• In both types, the lumens of the
distal convoluted tubules and
collecting ducts contain casts.
Hypertensive Vascular Disease
•Benign hypertension (diastolic > 90 mm Hg)
• Benign nephrosclerosis: granular surface of the kidney
results from small cortical scars
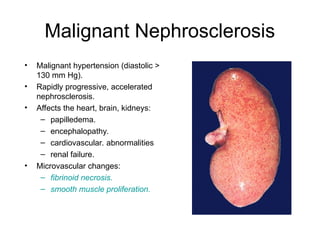
• Malignant hypertension (diastolic > 130 mm Hg):
vascular necrosis & hemorrhage with acute cardiac &
renal failure
40.
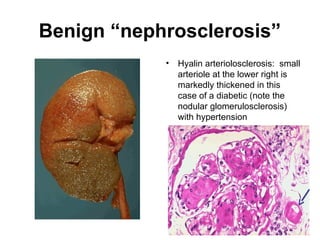
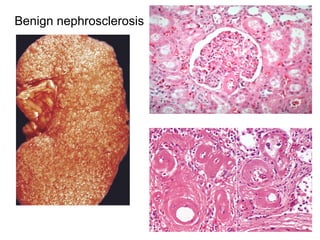
Benign “nephrosclerosis”
• Hyalinarteriolosclerosis: small
arteriole at the lower right is
markedly thickened in this
case of a diabetic (note the
nodular glomerulosclerosis)
with hypertension
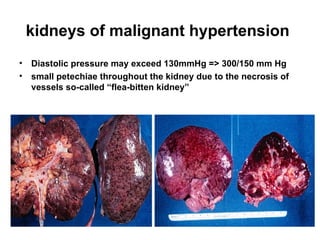
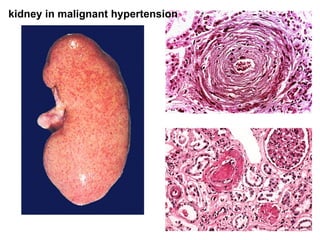
kidneys of malignanthypertension
• Diastolic pressure may exceed 130mmHg => 300/150 mm Hg
• small petechiae throughout the kidney due to the necrosis of
vessels so-called “flea-bitten kidney”
43.
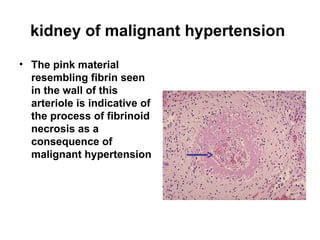
kidney of malignanthypertension
• The pink material
resembling fibrin seen
in the wall of this
arteriole is indicative of
the process of fibrinoid
necrosis as a
consequence of
malignant hypertension
44.
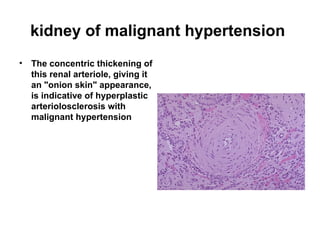
kidney of malignanthypertension
• The concentric thickening of
this renal arteriole, giving it
an "onion skin" appearance,
is indicative of hyperplastic
arteriolosclerosis with
malignant hypertension