Injuries that resultfrom direct contact
or exposure to any thermal, chemical,
electrical or radiation source are
termed as BURNS
Burn injuries occur when energy from a
heat source is transferred to the
tissues of the body.
4.
Thermal burn arecaused by exposure to or contact
with flame, hot liquids, semi liquids or steam.
a). Flame: e.g. clothing ignite (catch fire)
with fire
b).Flash(Spark): Explosion of combustible fuels
c).Scald(injury/blister): e.g. Hot bath water
Hot grease or liquids from cooking ,Steam burns,
microwave food
6.
Specific examples ofthermal burn
are those sustained in
residential fires, explosives,
scald injuries, clothing ignition
and ignition of poorly stored
flame able liquid petrol
8.
Chemical burn areresult of tissue
injury and destruction from
necrotizing substance
Chemical burns are caused by tissue
contact with strong acids, alkalies or
organic compounds
Chemical injuries to eyes and
inhalation of chemical fumes are
particularly serious
9.
Cont..
Chemical burns aremostly caused
by acids , however alkali burns also
occur
Alkali are more dangerous than
acids because alkali substance are
neutralized by tissue fluids Alkali
adhere (stick) to tissues, causing
protein hydrolic and liquefaction thus
damage continues until alkali
neutralized
10.
Cont..
Chemicals can producerespiratory
and systemic symptoms as well as
skin or eyes injuries
For example when chlorine is inhaled
toxic gas produce respiratory distress.
By products of burning substances e.g.
carbon are toxic to the sensitive
respiratory mucosa. Tissue destruction
may continue for up to 72 hours after
chemical injury
12.
Electrical injuries resultfrom coagulation necrosis
that is caused by intense heat generated by the
electrical energy as it passes through the body.
These injuries can result from contact with
exposure or faulty electrical wiring or high voltage
power lines.
It can also result from direct damage to nerves
and vessels causing tissues anoxia (absence of
oxygen) and death
Electrical contact with voltage greater than 40 is
potentially dangerous
14.
Radiation burn arecaused by exposure to
the radioactive service
These types of injuries have been
associated with nuclear accidents, the
use of ionizing radiation in industry.
A sun burn solar radiation from
prolonged exposure to ultraviolet rays is
also considered to be a type of radiation
burn.
16.
The treatment ofburn is related to the
severity of burn injury.
The severity of burn injury is determined
by:
Burn depth
Burn size
Burn location
Age of burn victim
General health of burn victim
Mechanism of injury
18.
Burn injuries areclassified as a
partial or full thickness
A). Partial Thickness
Partial thickness burn injuries are
classified as first and second
degree burns or superficial and
deep burn.
19.
Cont..
i.
ii.
Causes of Superficial(1st deg) Burn
Sunburn
Quick heat flash
In superficial burn pain sensation is
intact
Sign and Symptoms
a). Mild swelling
b). Erythaemia
c). Blenching on pressure
21.
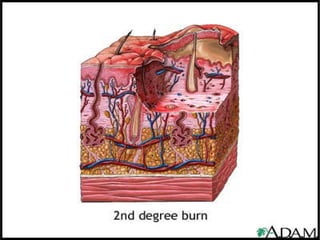
Causes of DeepBurn (2nd deg) Burn
The causes of deep burns / 2nd degree
are
a). Flame
b). Flash
c). Scald
d). Contact burns
In deep burn the epidermis and
dermis involved
23.
Sign and Symptomsof deep burn
1. Fluid filled vesicles that are red shinny. if,
vesicles are ruptured
2. Severe pain caused by nerve injury
3. Mild to moderate edema
Superficial burns heal in less than 21 days and
deep burns require more than 21 days
Healing rates vary with burn depth and
presence of infection
24.
B). Full Thickness
Fullthickness burn injuries are
classified as THIRD and Fourth
Degree burn
Causes of burn
Flame
Scald
Chemical
Electric current
25.
Cont…
Here all skinelements and nerve
endings are destroyed
Clinical appearance will be:
Dry
Waxy
White
Leathery (Rubbery)
Hard skin
26.
Cont…
1.
2.
3.
4.
Visible thromboses vessel
Insensitivityto pain and pressure
because of nerve destruction
There will be possible involvement
of muscles, tendons and bones
3rd degree require auto grafting and
4th degree require auto grafting and
amputation of extremity
28.
Burn Size Extent
Thesize of a burn (percentage of injured skin,
excluding first degree burn) is determined
by following techniques
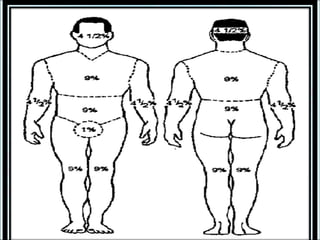
The Rule of Nine (9)
The rule of nine was introduced in the late
1940 as a quick assessment tool for
estimating burn size. The basis of this rule
is that the body divided into anatomic
sections, each of which represents 9% or a
multiple of 9% of the TBSA.
30.
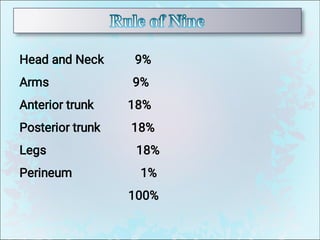
Head and Neck9%
Arms 9%
Anterior trunk 18%
Posterior trunk 18%
Legs 18%
Perineum 1%
100%
31.
The location ofburn wound has a direct
relationship to the severity of the burn injury.
Burn of the head, face, neck and
circumferential burns of the chest are
frequently associated with pulmonary
complications it may inhibit respiratory
functions by virtue of mechanical
obstruction secondary to edema.
These injuries may also indicate the
possibility of inhalation injury or respiratory
mucosal damage
Cont…
Burns of hands,feet, joints and eyes are of concern
because they make them self –care impossible.
Hands and feet are difficult to manage medically
because of superficial vascular and nerve supply
system
Burn involving the perinea area are prone to
infection due to auto contamination by urine
The burn of the buttock and genital are susceptible
to infection and may be source of emotional
conflict because of the pain involved possible
disfigurement.
35.
The client’s ageaffects the severity and outcome
of the burn. Mortality rate are higher for children
younger than 4 years and for client older than 65
years
Because of an immature immune system and
generally poor host defense mechanism an
infant is less able to cope with burn injuries
The older adult heals more slowly and has more
difficulty with rehabilitation than a child or
younger adult.
36.
Any patient withpre-existing cardiovascular,
pulmonary or renal disease has poorer prognosis
for recovery because of the tremendous demands
placed on the body by a burn injury
The patient with diabetes mellitus or peripheral
vascular disease is at high risk for gangrene and
poor healing , especially with foot and leg burns.
Patients who concurrently sustained fractures, head
injuries or other trauma has poorer prognosis for
recovery from the burn injury
37.
Mechanism of burninjury is an important factor
used to determine severity.
As stated earlier, in electrical injuries heat is
generated as the electricity travels through the
body resulting internal tissue damage. Here, the
voltage, type of current, AC or DC, contact site
and the duration of contact are important
consideration because they affect morbidity.
AC is worst than DC because it is associated with
cardiopulmonary arrest, ventricular fibrillation and
vertebral compression fractures
38.
1.
2.
3.
4.
Nursing care ofminor wounds include:
Wound assessment and initial care of
wound
Tetanus immunization
Pain management
Health education
39.
1.
2.
3.
Burn management canbe classified in
three phases
Emergent phase (Resuscitation)
The acute phase
The rehabilitative phase
40.
The emergent phasebegins at the
time of injury, with the pre hospital
care and concludes when capillary
integrity is restored, typically at 48 to
72 hours following injury.
The primary goals during the emergent
phase of recovery are directed
towards sustaining life through
prevention of hypovolemia burn.
41.
The intermittent /acutephase begins 48-72 hours after the
burn injury
In this phase continues attention is directed towards
continues assessment and maintenance of respiratory and
circulatory status, fluid and electrolyte balance and GI
function, infection prevention, burn wound care, pain
management , nutritional support are priorities in this stage
of burn.
Cautious administration of fluid and electrolyte continues
during this phase of burn care b/c of shift in the fluid from
interstitial to intravascular compartment, loss of fluid from
large burn wound
Blood component are administered as needed
42.
Central venous, peripheralarterial, or pulmonary artery
thermo dilution catheter may be required for monitoring
venous and arterial pressure, pulmonary artery pressure and
cardiac output.
However, invasive lines are avoided unless essential
because they provide an additional port for infection in an
already greatly compromised patient.
Infection progressing to septic shock is the major cause of
death in patient who has survived the first few days after
the a major burn
The infection that begins within the burn site may spread to
the blood stream
43.
1.
2.
3.
4.
5.
The rehabilitation phasebegins immediately after
the burn has occurred-often extend years after
injury
Patient increasingly focus on alternations in self
image life style that may occur
Wound healing, psychological support and
restoring maximum functional activity remain
priorities
Reconstructive surgery to improve body
appearance and functions may be needed
Family members also need support and guidance
44.
Impaired gas exchangerelated to carbon mono oxide
poisoning, smoke inhalation and upper airway obstruction
secondary to Burn
Ineffective airway clearance related to edema and effect
of smoke inhalation
Fluid volume deficit related to increase capillary
permeability evaporative losses from the burn wound
Hypothermia related to loss of skin microcirculation
open wound
Pain related to tissue and nerve injury
Anxiety related to fear and emotional impact of burn injury


















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





