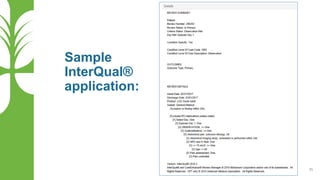
1) Stuart, a 79-year-old male with multiple comorbidities, presented with signs of an ischemic stroke. He required intensive monitoring, treatment with anticoagulants and management of complications.
2) On episode day 4, Stuart developed pneumonia requiring oxygen supplementation and nebulizer treatments. He continued physical, occupational and speech therapy for his stroke.
3) Based on the ongoing intensive interventions and management of complications, Stuart's inpatient admission remained medically necessary.















![The PPS [Prospective Payment System] to PDPM Pendulum: An Analysis of PDPM Co...](https://cdn.slidesharecdn.com/ss_thumbnails/ahlapresentationppspdpmpendulumv3cb-200311184156-thumbnail.jpg?width=640&height=640&fit=bounds)