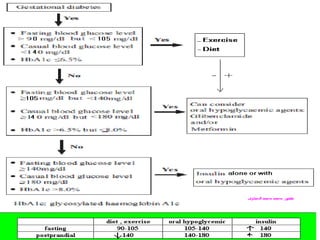
This document discusses gestational diabetes, including its definition, epidemiology, consequences for both mother and fetus, screening recommendations, management, and controversies around diagnostic criteria. Some key points:
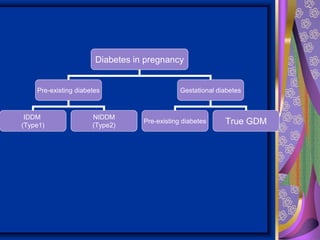
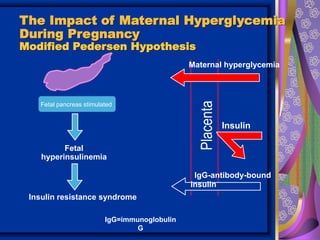
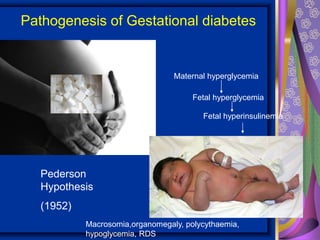
- Gestational diabetes is defined as carbohydrate intolerance first recognized during pregnancy and can include undiagnosed preexisting diabetes.
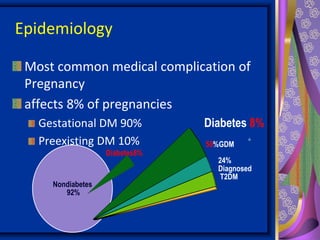
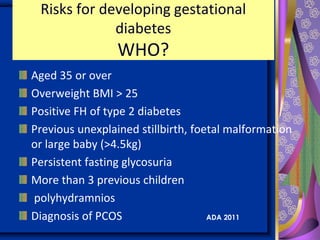
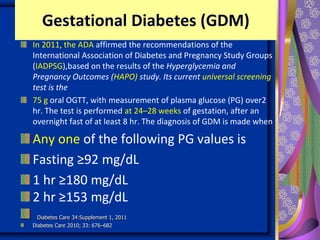
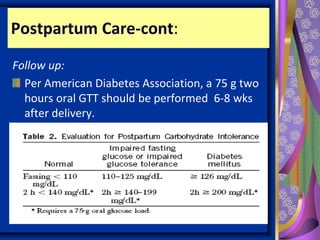
- It affects 2-9% of pregnancies and screening is recommended for at-risk women between 24-28 weeks using a 75g oral glucose tolerance test.
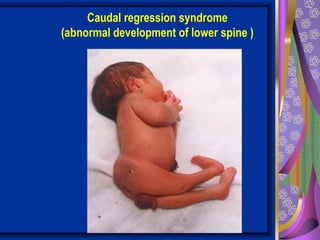
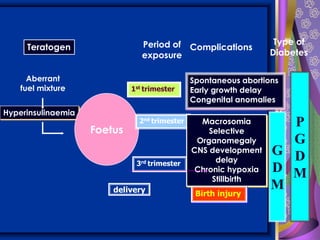
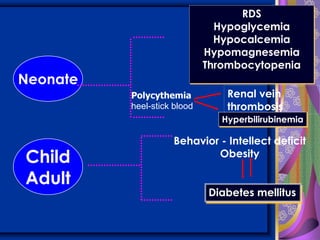
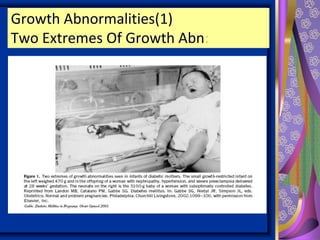
- Risks for the fetus include macrosomia, jaundice, and hypoglycemia. Risks for the mother include preeclampsia, infections, and long-term risk of type 2 diabetes.