Download to read offline

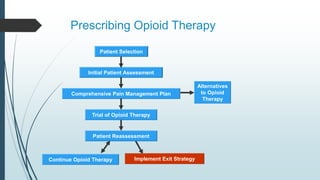

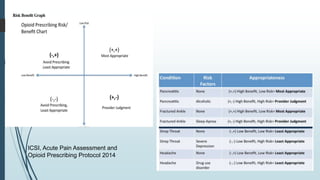

This document provides information on best practices for prescribing opioid therapy and managing pain patients, including key facts on the pain management epidemic. It discusses definitions of chronic pain and addiction. Guidelines are provided on initial patient assessment, implementing opioid therapy if appropriate, identifying addiction risks, prescribing protocols, urine drug testing protocols, and legislation related to prescription drug monitoring programs. The goal is to provide physicians with tools and guidelines for safely and effectively managing patients with chronic pain.

















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)





