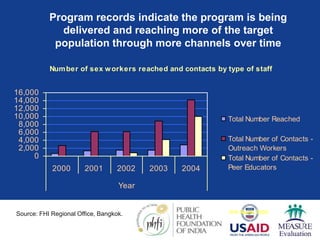
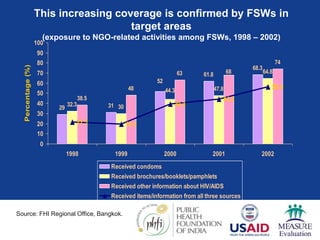
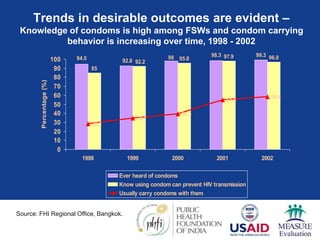
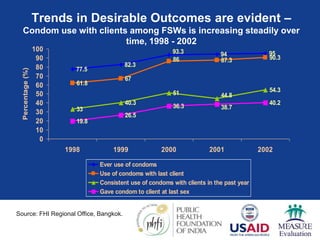
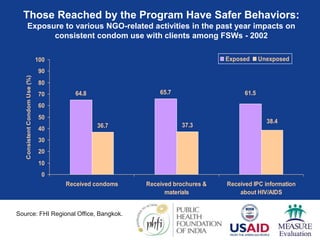
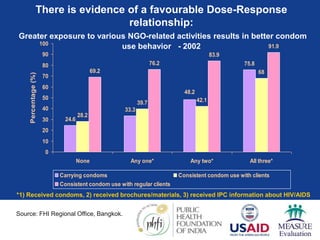
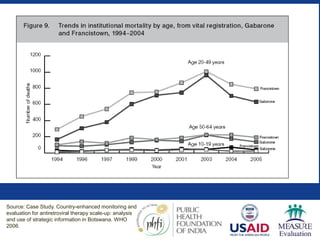
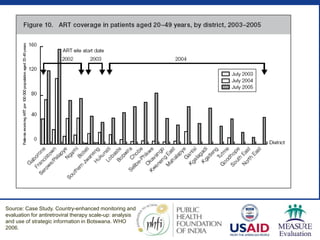
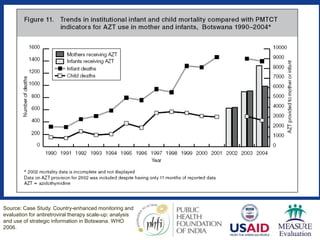
This document discusses data triangulation, which involves analyzing data from multiple sources to increase the validity of evaluation findings. It provides examples of data sources that can be used, such as service statistics, surveys, and qualitative research. When triangulating data, considerations include whether the data is representative and if the time frames align. The document then summarizes two case studies that successfully used data triangulation. In Nepal, condom use among female sex workers increased as exposure to prevention programs grew, showing a dose-response relationship. In Botswana, mortality reductions were linked to increased antiretroviral treatment coverage. Triangulating diverse data sources can provide compelling evidence of public health program impact.













![M & e training [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/metrainingautosaved-130520213341-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









































