Introduction to Thrombosis
Thrombosisis the formation of a blood
clot within a blood vessel.
Understanding its pathogenesis is
crucial for recognizing risk factors and
developing effective treatments.
Thrombosis occurs when blood clots form
inappropriately, obstructing blood flow. This can
lead to serious conditions such as heart attacks and
strokes.
3.
Types of Thrombosis
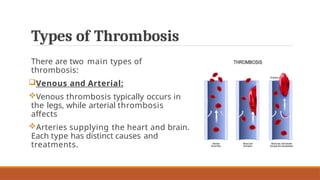
Thereare two main types of
thrombosis:
Venous and Arterial:
Venous thrombosis typically occurs in
the legs, while arterial thrombosis
affects
Arteries supplying the heart and brain.
Each type has distinct causes and
treatments.
5.
VIRCHOW’S TRIAD
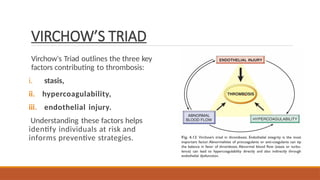
Virchow's Triadoutlines the three key
factors contributing to thrombosis:
i. stasis,
ii. hypercoagulability,
iii. endothelial injury.
Understanding these factors helps
identify individuals at risk and
informs preventive strategies.
6.
Role of EndothelialCells
Endothelial cells line blood vessels
and play a vital role in maintaining
vascular health.
Damage to these cells can trigger
thrombosis by promoting platelet
activation and clot formation.
Their function is crucial in preventing
unwanted
7.
Hypercoagulability:
Definition:
Hypercoagulability refers toany alteration of the coagulation pathways that pre-disposes to
thrombosis.
Causes:
1. Primary (Genetic):-
Factor V Leiden mutation (resistance
to protein C)
Prothrombin gene mutation
Deficiency of antithrombin III,
protein C, or protein S .
Secondary (Acquired):
Prolonged bed rest or immobilization
Myocardial infarction
Disseminated intravascular coagulation
Heparin-induced thrombocytopenia
8.
Mechanism & ClinicalSignificance of
Hypercoagubility:
Mechanism:
Increased procoagulant activity.
Reduced anticoagulant activity.
Reduced fibrinolysis
Clinical Significance:
Major risk factor for venous thrombosis.
Usually presents as deep vein thrombosis(DVT) or pulmonary embolism.
Important component of Virchow's triad.
9.
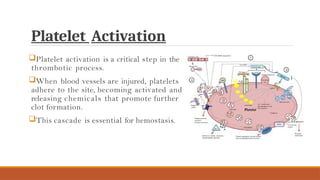
Platelet Activation
Platelet activationis a critical step in the
thrombotic process.
When blood vessels are injured, platelets
adhere to the site, becoming activated and
releasing chemicals that promote further
clot formation.
This cascade is essential for hemostasis.
10.
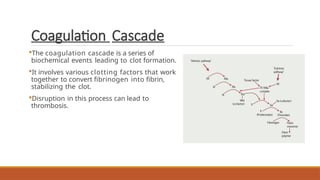
Coagulation Cascade
The coagulationcascade is a series of
biochemical events leading to clot formation.
It involves various clotting factors that work
together to convert fibrinogen into fibrin,
stabilizing the clot.
Disruption in this process can lead to
thrombosis.
11.
Risk Factors forThrombosis
Several risk factors contribute to thrombosis, including:
i. obesity,
ii. smoking,
iii. diabetes,
iv. prolonged
v. immobility.
12.
Morphology of Thrombosis
•Thrombiare focally attached to the vessel wall and propagate toward the heart; the propagating
end is loosely attached and prone to embolization.
•Lines of Zahn: laminated appearance with alternating pale platelet–fibrin layers and dark RBC-rich
layers; seen only in antemortem thrombi formed in flowing blood.
•Mural thrombi: thrombi in cardiac chambers or aorta; associated with abnormal myocardial
contraction, endomyocardial injury, atherosclerotic plaques, or aneurysms.
•Arterial thrombi: usually occlusive, platelet-rich, commonly over ruptured atherosclerotic plaques;
may also occur with vasculitis or trauma.
13.
Morphology of Thrombosis
•Venousthrombi (phlebothrombosis): almost always occlusive, form long casts in veins, RBC-rich (“red”
or stasis thrombi); most common in deep veins of lower limbs.
•Postmortem clots vs thrombi: postmortem clots are gelatinous, non-adherent, “chicken-fat”
appearance; true thrombi are firm, attached, with fibrin strands.
•Valve thrombi (vegetations):
•Infective endocarditis – large infected vegetations
•Nonbacterial thrombotic endocarditis – sterile vegetations in hypercoagulable states
•Libman–Sacks endocarditis – sterile verrucous vegetations in SLE
14.
Thrombosis and Inflammation
Inflammatorycytokines can enhance platelet reactivity and promote
thrombus formation, suggesting that managing inflammation may be
key in preventing thrombosis.
Diagnosis of Thrombosis:
Diagnosis of thrombosis typically involves clinical evaluation and
imaging techniques such as ultrasound or CT scans. Blood tests
measuring clotting factors can also aid in assessing the risk and
presence of thrombosis.
15.
FATE OF THETHROMBUS:
•Propagation: Thrombus enlarges by deposition of platelets and fibrin → ↑ risk of vascular occlusion and embolism.
•Embolization: Part or whole thrombus detaches and travels through circulation to a distant site.
•Dissolution:
•Recent thrombi may undergo fibrinolysis and complete resolution.
•Older thrombi become resistant to lysis due to fibrin polymerization → fibrinolytic therapy effective only early.
•Organization and Recanalization:
•Ingrowth of endothelial cells, smooth muscle cells, and fibroblasts.
•Formation of capillary channels partially restores blood flow.
•Thrombus may become incorporated into vessel wall as connective tissue.
•Complications:
•Central enzymatic digestion may occur.
•Bacterial infection can lead to mycotic aneurysm.
16.
Disseminated Intravascular Coagulation
(DIC)
•DICis widespread thrombosis in the microcirculation.
•Onset may be acute or insidious.
•Seen in conditions such as obstetric complications and advanced malignancy.
•Causes consumption of platelets and coagulation factors → consumptive
coagulopathy.
•Fibrinolysis is simultaneously activated, increasing bleeding tendency.
•The net result is that excessive clotting and bleeding may co-exist in the
same patient.
17.
Treatment Options
Treatment forthrombosis may include:
i. anticoagulants,
ii. thrombolytics,
iii. lifestyle modifications.
Early intervention is critical to prevent
complications such as pulmonary embolism
or post- thrombotic syndrome
18.
Conclusion
Understanding the pathogenesisof
thrombosis is vital for prevention
and treatment. By recognizing risk
factors and mechanisms, healthcare
professionals can implement
effective strategies to mitigate the
impact of this serious condition.