areas of the BSSW curricareas of the BSSW curriculumareas of the BSSW curriculumareas of the BSSW curriculumareas of the BSSW curriculumareas of the BSSW curriculumulum
I. Psychoanalytic/ PsychodynamicTheories
+ The unconscious is important.
People use defense mechanisms
when uncomfortable.
Utilizes the concept of transference
and countertransference.
People find relief through catharsis.
Psychoanalytical and Psychodynamic
Therapies
Psychoanalyticaland psychodynamic
therapies are based on an individual's
unconscious thoughts and perceptions
that have developed throughout their
childhood, and how these affect their
current behaviour and thoughts.
The past: Current problems stem from
unresolved issues that occurred in early
childhood.
7.
Psychoanalytic Key Concepts
Influence of the past
Experiences of first 6 years of life are critical
The Unconscious
Thoughts, feelings, experience kept out of awareness
Anxiety and ego defenses
Dynamics of anxiety are related to concept of defense
Resistance
Unique meaning of resistance as a key defense
Transference and countertransference
How these operate in a counseling relationship.
Theory and Practice of Group Counseling—Chapter 6 (1)
8.
Psychoanalysis
Psychoanalysis was developed
bySigmund Freud. Through free
associations, dreams or
fantasies, clients can learn how
to interpret deeply buried
memories or experiences that
may be causing them distress.
9.
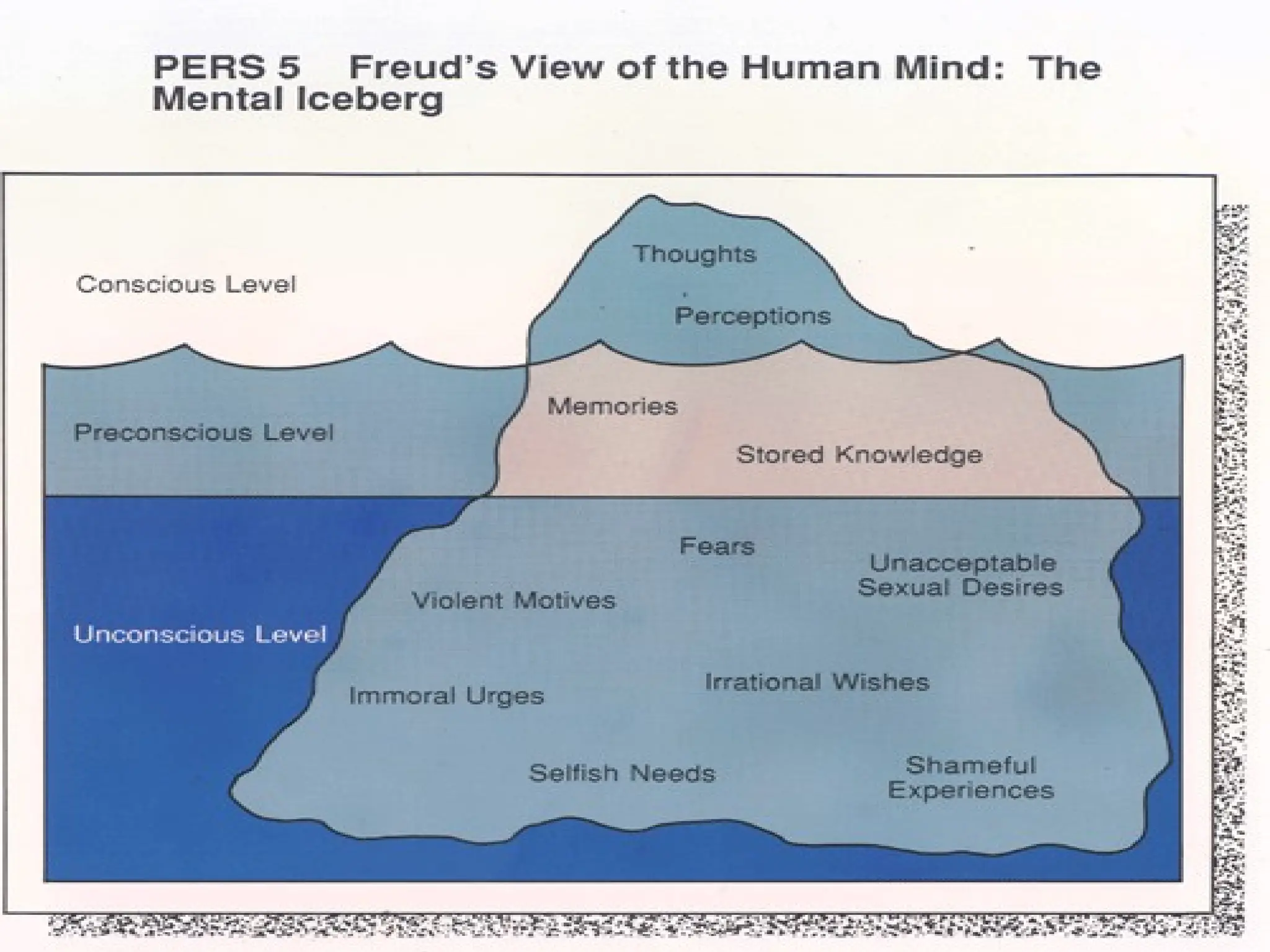
The unconscious mind
The unconscious mind is a reservoir of
feelings, thoughts, urges, and memories
that are outside of our conscious
awareness. Most of the contents of the
unconscious are unacceptable or
unpleasant, such as feelings of pain,
anxiety, or conflict. According to Freud, the
unconscious continues to influence our
behavior and experience, even though we
are unaware of these underlying
influences.
11.
Psychoanalytic
Many explanations for
seeminglyirrational behavior
can be found by analyzing the
conflicting sexual and
aggressive needs, fears, and
wishes that are housed in the
unconscious.
12.
Psychoanalytic
This theory describes3 basic
structures of personality:
1.) Id - the sexual and aggressive
impulses – operates on “pleasure-
principle.”
2.) Ego - reality-oriented functions.
3.) Superego - the moral, ethical
principles.
13.
Id
Basic psychic
energyand
motivations
Operates to
demands of
Pleasure
Principle - strive
to satisfy desires
and reduce inner
tension
14.
Ego
Deals withreal
world
Operates to
demands of
Reality
Principle solves
problems by
planning & acting
What happens whenthe ego
cannot deal with the demands of
our desires, the constraints of
reality, and our own moral
standards?
According to Freud, we develop
anxiety. Anxiety acts as a signal
to the ego that things are not
going right.
17.
Defense Mechanisms
In orderto deal with
anxiety, Freud believed
that defense mechanisms
helped shield the ego from
the conflicts created by the
id, superego and reality.
18.
There are anumber of
defense mechanisms that
have been described by
researchers.
Sigmund Freud's daughter,
Anna Freud described ten
different defense
mechanisms used by the ego.
19.
Denial
Denial isprobably one of the best known
defense mechanisms, used often to describe
situations in which people seem unable to face
reality or admit an obvious truth (i.e. "He's in
denial.").
Denial is an outright refusal to admit or
recognize that something has occurred or is
currently occurring.
Drug addicts or alcoholics often deny that they
have a problem, while victims of traumatic
events may deny that the event ever occurred.
20.
Repression
Repression actsto keep information out of
conscious awareness. However, these
memories don't just disappear; they continue to
influence our behavior. For example, a person
who has repressed memories of abuse
suffered as a child may later have difficulty
forming relationships.
Sometimes we do this consciously by forcing
the unwanted information out of our
awareness, which is known as suppression,
but it is usually believed to occur
unconsciously.
21.
Displacement
Displacement involvestaking out our
frustrations, feelings and impulses on
people or objects that are less
threatening.
Rather than express our anger in ways
that could lead to negative consequences
(like arguing with our boss), we instead
express our anger towards a person or
object that poses no threat (such as our
spouses, children or pets).
22.
Sublimation
Sublimation isa defense mechanism that
allows us to act out unacceptable impulses by
converting these behaviors into a more
acceptable form.
For example, a person experiencing extreme
anger might take up kick-boxing as a means of
venting frustration. Freud believed that
sublimation was a sign of maturity that allows
people to function normally in socially
acceptable ways.
23.
Projection
Projection is adefense mechanism
that involves taking our own
unacceptable qualities or feelings and
ascribing them to other people.
For example, if you have a strong
dislike for someone, you might
instead believe that he or she does
not like you.
24.
Intellectualization
Intellectualization worksto reduce anxiety by
thinking about events in a cold, clinical way.
This defense mechanism allows us to avoid
thinking about the stressful, emotional aspect
of the situation and instead focus only on the
intellectual component.
For example, a person who has just been
diagnosed with a terminal illness might focus
on learning everything about the disease in
order to avoid distress and remain distant from
the reality of the situation.
25.
Rationalization
Rationalization isa defense mechanism that
involves explaining an unacceptable behavior
or feeling in a rational or logical manner,
avoiding the true reasons for the behavior.
For example, a person who is turned down for
a date might rationalize the situation by saying
they were not attracted to the other person
anyway, or a student might blame a poor exam
score on the instructor rather than his or her
lack of preparation.
26.
Regression
When confrontedby stressful events, people
sometimes abandon coping strategies and
revert to patterns of behavior used earlier in
development. For example, an individual
fixated at an earlier developmental stage might
cry or sulk upon hearing unpleasant news.
An individual fixated at the oral stage might
begin eating or smoking excessively, or might
become very verbally aggressive.
A fixation at the anal stage might result in
excessive tidiness or messiness.
27.
Reaction Formation
Reactionformation reduces anxiety by
taking up the opposite feeling, impulse or
behavior. An example of reaction
formation would be treating someone you
strongly dislike in an excessively friendly
manner in order to hide your true feelings.
They are using reaction formation as a
defense mechanism to hide their true
feelings by behaving in the exact opposite
manner.
28.
Other Defense Mechanisms
Acting out - The individual copes with stress by
engaging in actions rather than reflecting upon
internal feelings.
Affiliation - Involves turning to other people for
support.
Aim inhibition - The individual accepts a
modified form of their original goal (i.e.
becoming a high school basketball coach
rather than a professional athlete.)
Altruism - Satisfying internal needs through
helping others.
29.
Avoidance -Refusing to deal with or
encounter unpleasant objects or situations.
Compensation - Overachieving in one area
to compensate for failures in another.
Humor - Pointing out the funny or ironic
aspects of a situation.
Passive-aggression - Indirectly expressing
anger.
30.
While all defensemechanisms
can be unhealthy, they can also
be adaptive and allow us to
function normally.
The greatest problems arise when
defense mechanisms are
overused in order to avoid dealing
with problems.
31.
Psychoanalytic Techniques
FreeAssociation (Talking therapy)
Individual reports immediately without censoring any
feelings or thoughts
Interpretation
Counselor points out, explains, and teaches the
meanings of whatever is revealed
Dream Analysis
Dreams are the “royal road to the unconscious”
Dreams can be productively worked with in a group
setting
Client can share and explore dreams during the
counseling session
Theory and Practice of Group Counseling—Chapter 6 (5)
32.
Evaluation of PsychoanalyticApproach
Contributions and strengths of
the approach
Important to understand how
past contributes to present
problem
Provides a conceptual
framework to understand anxiety
and defense
Theory and Practice of Group Counseling—Chapter 6 (9)
33.
Limitations of theapproach
Limitations based on long-term
approach for many clients
Critique from feminist
perspective – too masculine!
The approach has not given full
attention to social and cultural
factors
34.
II. COGNITIVE- Behavioral:
This is based on the premise
that primary learning comes
from experience.
The initial concern in therapy
is to help the client analyze
behavior, define problems,
and select goals.
35.
Behavioural Therapy
Behavioural Therapyfocuses on an
individual's learned, or conditioned,
behaviour and how this can be
changed. The approach assumes that
if a behaviour can be learned, then it
can be unlearned (or reconditioned)
so is useful for dealing with issues
such as phobias or addictions.
36.
BEHAVIOURAL THEORIES
• Basicassumption of behavioural
theories is that maladaptive
behaviours are learned and can be
unlearned, and that new, more
adaptive behaviours can be learned
• Has been applied to a wide range
of disorders and problems
37.
BEHAVIOURAL THEORIES
Operant conditioning
A.Reinforcement – leads to an increase in
the desirable behaviour preceding the
reinforcer
• positive * negative
B. Punishment – used to decrease an
undesirable behavior
• positive * negative
39.
Cognitive:
We define thisas any therapy
that is based on the belief that
our thoughts are directly
connected to how we feel. The
cognitive therapies include
Rational-Emotive, Cognitive-
Behavioral, Reality, and
Transactional Analysis.
41.
COGNITIVE THEORIES
Aaron Beck– psychological
problems stem from distorted
thinking based on underlying
cognitive schemata
Cognitive schemata – ways of
viewing self, world, past, future
42.
Cognitive therapy -
therapistchallenges
client’s distorted thinking
through a process of
checking beliefs against
reality – evidence-
gathering approach
43.
Cognitive Behavioural Therapy(CBT)
Cognitive Behavioural Therapy
(CBT) combines cognitive and
behavioural therapies. The
approach focuses on thoughts,
emotions, physical feelings and
actions, and teaches clients how
each one can have an affect on
the other.
44.
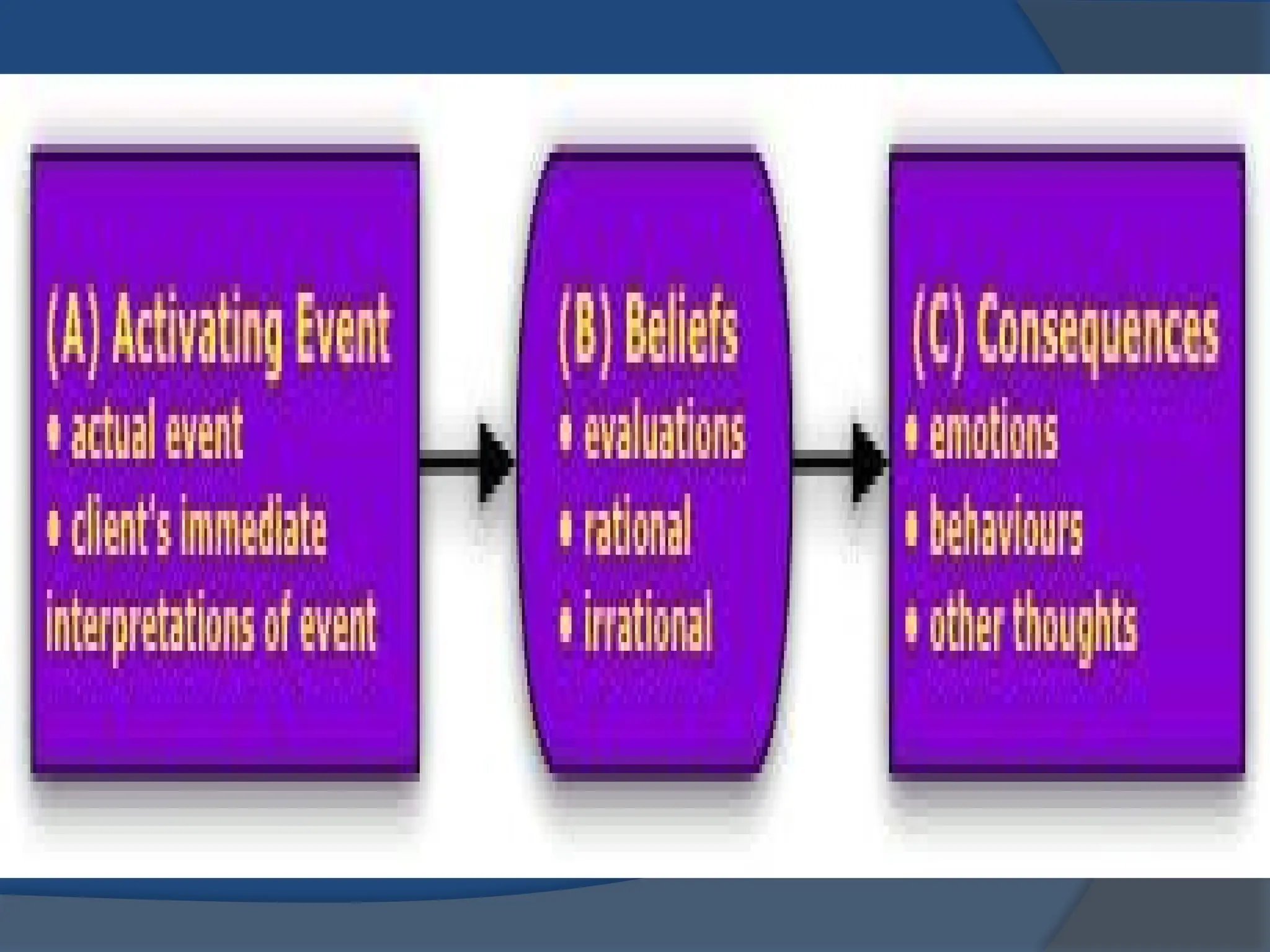
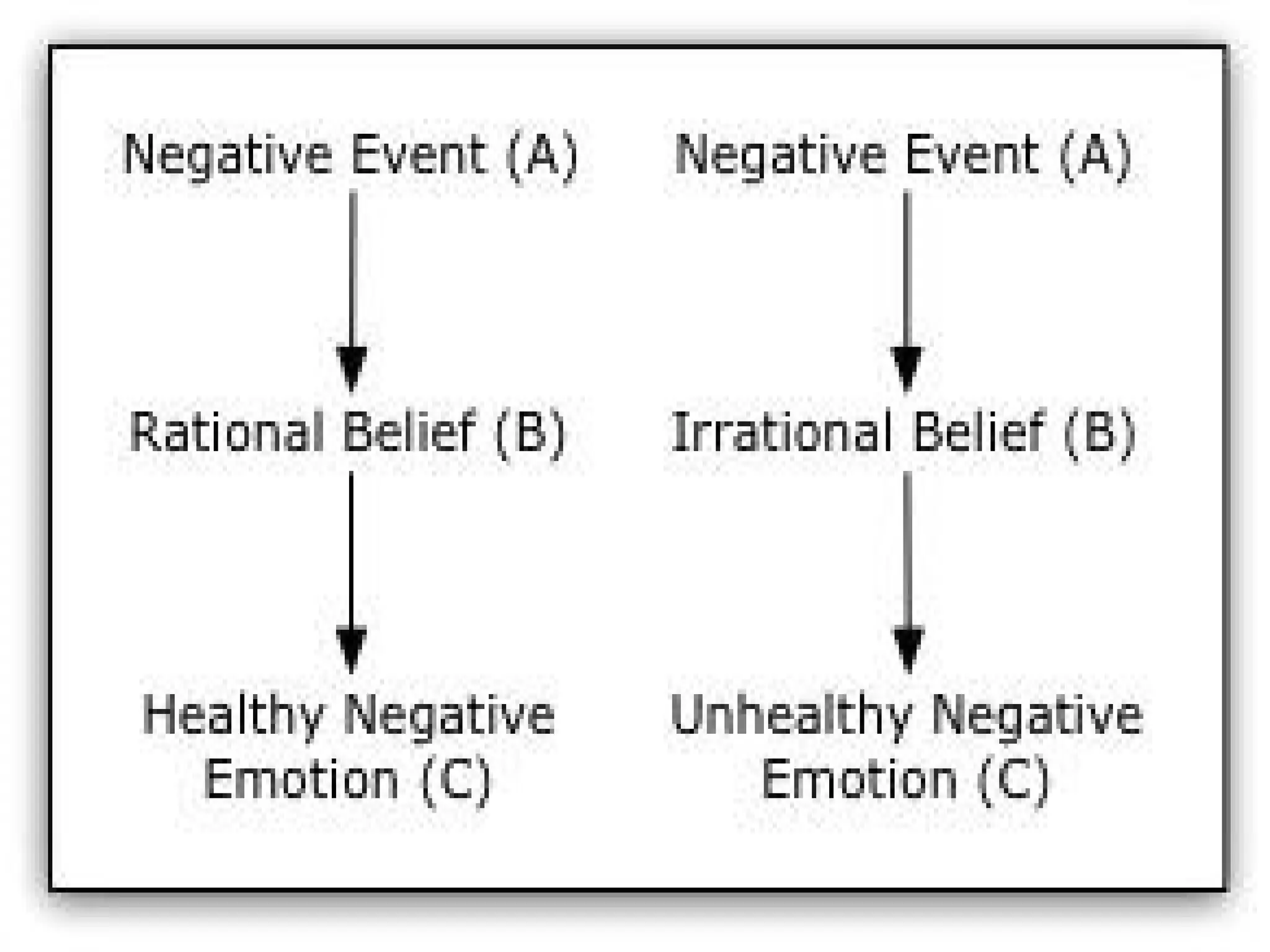
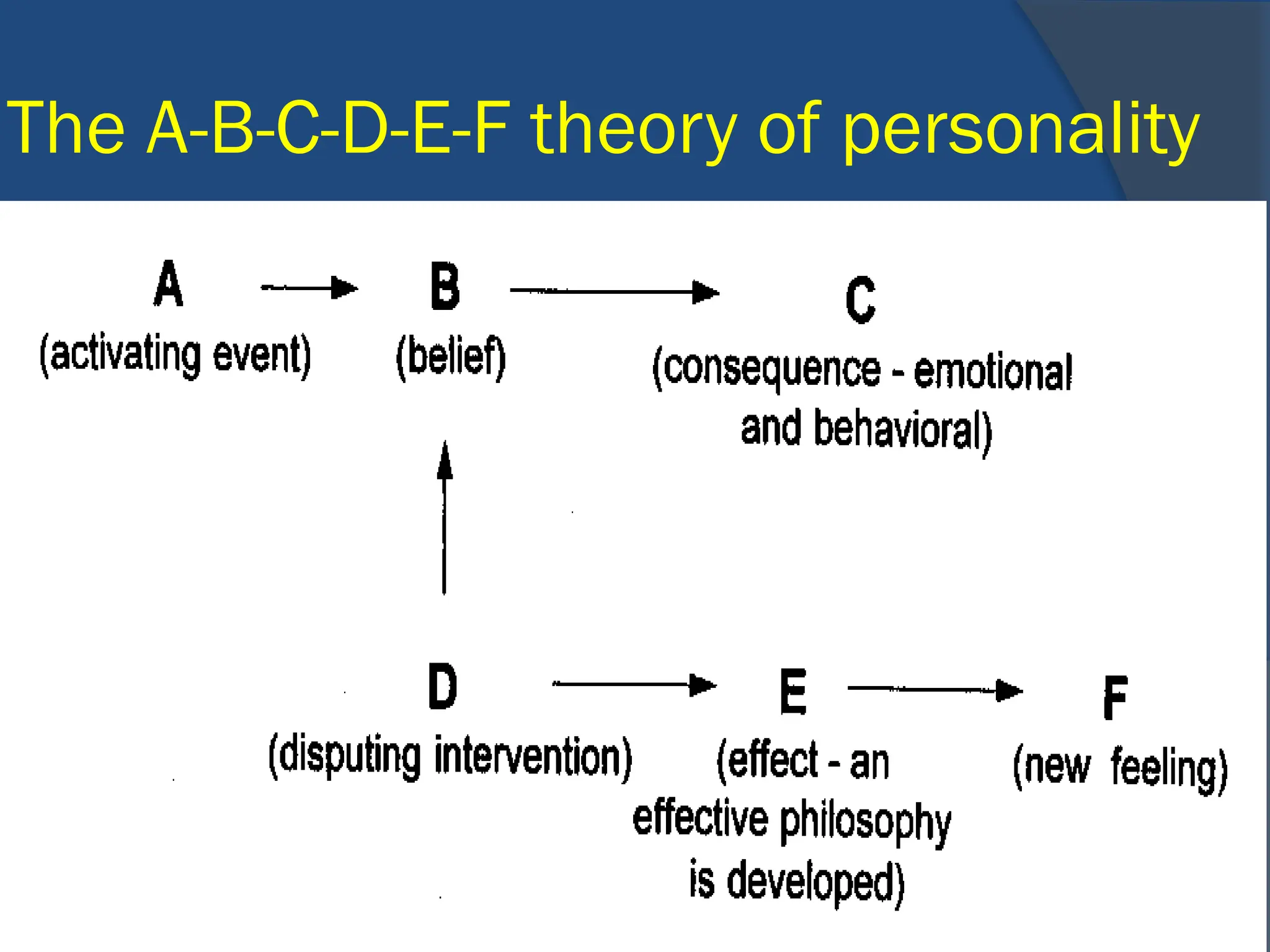
Cognitive BehavioralTherapy (ABC
Method) could be described as “as I
think, so I feel (and do)!” In any given
situation you have:
Activating Event – the actual event and
the client’s immediate interpretations of
the event.
Beliefs about the Event - this evaluation
can be rational or irrational.
Consequences - how you feel and what
you do or other thoughts.
46.
In the charts,previous and
after this slide, you can see
how that when a negative
event happens, one can
interpret it positively or
negatively. How one interprets
it affects how one feels, thinks
and behaves.
,The role ofthe Social
worker in cognitive
behavioral therapy is
to challenge false
beliefs- “The Lies We
Tell Ourselves”
50.
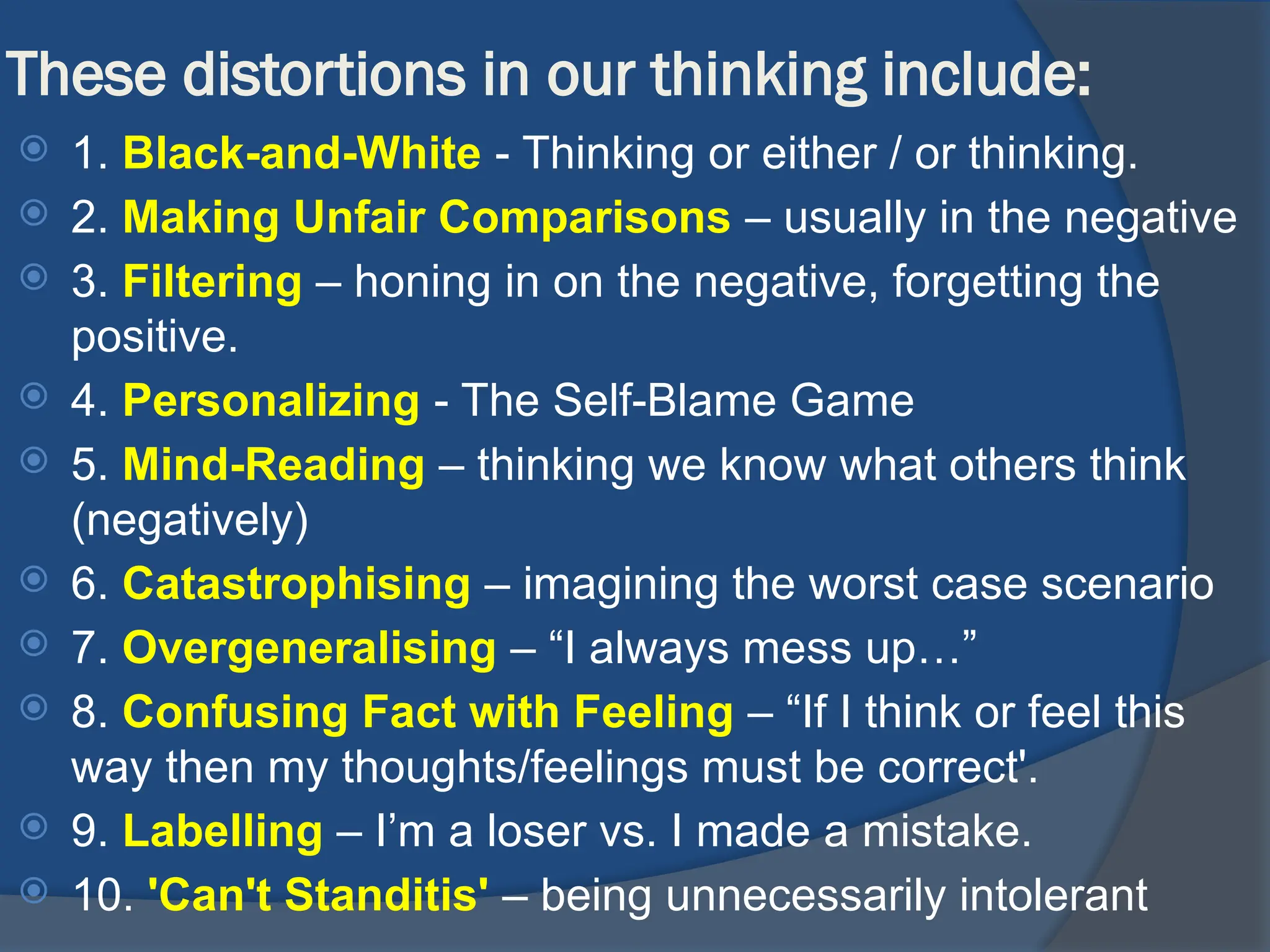
These distortions inour thinking include:
1. Black-and-White - Thinking or either / or thinking.
2. Making Unfair Comparisons – usually in the negative
3. Filtering – honing in on the negative, forgetting the
positive.
4. Personalizing - The Self-Blame Game
5. Mind-Reading – thinking we know what others think
(negatively)
6. Catastrophising – imagining the worst case scenario
7. Overgeneralising – “I always mess up…”
8. Confusing Fact with Feeling – “If I think or feel this
way then my thoughts/feelings must be correct'.
9. Labelling – I’m a loser vs. I made a mistake.
10. 'Can't Standitis' – being unnecessarily intolerant
51.
WDEP
W Wants -What do you want to be and do?
D Doing and Direction - What are you doing?
E Evaluation - Does your present behavior
have a reasonable chance of getting you what
you want?
P Planning – identify ways to fulfill their wants
and needs.
52.
SAMIC
S Simple- Easy to understand, specific and
concrete
A Attainable - Within the capacities and motivation of
the client
M Measurable -Are the changes observable and
helpful?
I Immediate and Involved - What can be done
today? What can you do?
C Controlled - Can you do this by yourself or will you
be dependent on others?
53.
III. Humanistic Theories
HumanisticTherapies focus on
self-development, growth and
responsibilities. They seek to
help individuals recognise their
strengths, creativity and choice in
the 'here and now'.
54.
Person-Centered (Rogerian):
Foundedby Carl Rogers in the 1940's,
like Adlerian therapy, a basic premise is
that we are all "becoming;" we are all
moving towards self-actualization.
Rogers believed that each of us has the
innate ability to reach our full potential.
As infants we are born with it, but
because of early experiences, we may
lose our connection to it.
55.
The self conceptwe develop in
response to our early experiences
may tend to alienate us from our true
self. In this theory there is no such
thing as mental illness. It is just a
matter of being disconnected from
our self-potential. This therapy is
often considered the most optimistic
approach to human potential.
56.
The basic premisebehind Client
Centered (Rogerian) counseling is
that the client is the best authority on
her / his own experience, and it
asserts that the client is fully capable
of changing and growing into all that
the client can and wants to be.
However, the client – like all of us -
needs favorable conditions in which
to blossom and bloom.
To be genuinethe therapist
must strive to be transparent,
open, willing to express at
opportune times their own
identity in the relationship.
There is no hiding behind
expertise or degrees.
Therapists must be constantly
doing their own inventory.
Empathic understanding
is basedon the therapist's
ability to see the world
through the client's eyes, to
move into the client's world
at the deepest levels and
experience what the client
feels.
63.
Person-Centred Counseling (or
“Rogerian”counseling)
Person-Centred Counselling
focuses on an individual's self
worth and values. Being valued as
a person, without being judged, can
help an individual to accept who
they are, and reconnect with
themselves.
64.
In Client-Centered (Rogerian)
counseling,the counselor
provides the growth-promoting
climate and the client is then free
and able to discover and grow as
she/he wants and needs to.
Prevailing characteristics of the
session are active listening,
empathy, acceptance.
65.
The Existential Approach
(Whyam I Here?) is also known as
“Meaning Therapy.” As Viktor Frankl
puts it, “He who knows the ‘why’ for
his existence will be able to bear
almost any ‘how.’” Therapy is
concerned with creating one’s
identity and establishing meaningful
relationships with others.
66.
The Capacity forSelf-Awareness
The greater our awareness, the greater our
possibilities for freedom
Awareness is realizing that:
We are finite—time is limited
We have the potential, the choice, to act or not to
act
Meaning is not automatic—we must seek it
We are subject to loneliness, meaninglessness,
emptiness, guilt, and isolation
Main purpose of an existential therapy is to increase
awareness
Theory and Practice of Group Counseling—Chapter 9 (2)
67.
The Search forMeaning
Like pleasure, meaning must be
pursued indirectly.
Struggle to find sense of significance and
purpose in life is part of human existence
“The will to meaning” is our primary
striving
Life is not meaningful in itself; the individual
must create and discover meaning
Theory and Practice of Group Counseling—Chapter 9 (4)
68.
Commonalities Among CounselingApproaches
All theories state the belief that people
can change.
Most theories recognize that behavior is
not strictly caused by past incidents but
is also influenced by the present and
hopes for the future.
All theories aim to reduce the suffering
of the client.
Brief Therapies:
While mosttherapy
approaches have developed
short term versions (often in
response to the demands of
managed care), one specific
model is called SOLUTION-
FOCUSED BRIEF THERAPY.
71.
This shortterm work is based on:
1. focusing on solutions instead of
problems,
2. Exceptions suggest solutions, i.e. "We
fight all the time." "Think of a time
recently when you weren't fighting."
3. Change is occurring all the time.
4. Small changing leads to large
changing.
5. People have all they need to solve
their problems.
72.
SOLUTION-FOCUSED BRIEF THERAPY
Thepremise is that if one does a
step by step process, the client can
find quick solutions to whatever may
be facing them.
Like the cognitive-behavioral
therapies this short term therapy
usually involves homework and
clearly defined goals.
73.
Solution-Focused Therapy
(Wheredo I want to be?) focuses on
what clients want to achieve through
therapy rather than on the problem(s)
that made them seek help. The
approach does not focus on the past, but
instead, focuses on the present and
future. The client is asked to envision
how the future will be different when the
problem is no longer present.
Techniques for SFtherapy
1. Looking for previous solutions
SF social workers have learned that most
people have previously solved many
problems and probably have some ideas
of how to solve the current problem. To
help clients see these potential solutions
they may ask, "What did you (or others)
do that was helpful in the past?"
76.
2. Present andfuture-focused questions vs.
past-oriented focus
The questions asked by SF social workers are
usually focused on the present or on the future.
This reflects the basic belief that problems are
best solved by focusing on what is already
working, and how a client would like their life to
be, rather than focusing on the past and what
isn’t wanted. For example, they may ask, "What
will you be doing in the next week that would
indicate to you and other that you are continuing
to make progress?"
77.
3. Compliments
Validatingwhat clients are already doing well,
and acknowledging how difficult their problems
are encourages the client to change while
giving the message that the counselor has
been listening and cares. In SF therapy,
compliments are often conveyed in the form of
appreciatively toned questions of “How did you
do that?” that invite the client to self-
compliment by virtue of answering the
question.
78.
4. Inviting theclients to do more of what is
working.
SF social workers invite the client to
do more of what has previously
worked, or to try changes they have
brought up which they would like to
try – frequently called "an
experiment.“
"How’s that working for you?"
79.
Eclectic or integrativeTherapy:
This is essentially a
common sense approach to
helping people by tailoring
therapy to the needs of the
individual client..
80.
Eclectic or IntegrativeTheory
Putting It All Together
Many clinicians use three or four different theories in
their practice.
Some look to common elements within all theories.
Some ascribe to technical eclecticism or integrate
several theories into one.
Some believe in specific treatments for specific issues
or symptoms.
81.
Integrative Theory
Why IntegrateTheories?
Because one theory does not fit all
people or all situations.
It enables a social worker to see each
client as unique and apply theories that
fit that client in regard to culture,
presenting issue, and diversity.