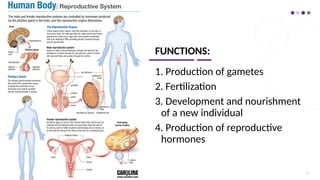
FUNCTIONS:
1. Production ofgametes
2. Fertilization
3. Development and nourishment
of a new individual
4. Production of reproductive
hormones
2
3.
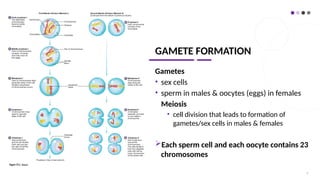
GAMETE FORMATION
Gametes
• sexcells
• sperm in males & oocytes (eggs) in females
Meiosis
• cell division that leads to formation of
gametes/sex cells in males & females
Each sperm cell and each oocyte contains 23
chromosomes
3
4.
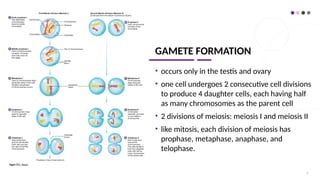
GAMETE FORMATION
• occursonly in the testis and ovary
• one cell undergoes 2 consecutive cell divisions
to produce 4 daughter cells, each having half
as many chromosomes as the parent cell
• 2 divisions of meiosis: meiosis I and meiosis II
• like mitosis, each division of meiosis has
prophase, metaphase, anaphase, and
telophase.
4
5.
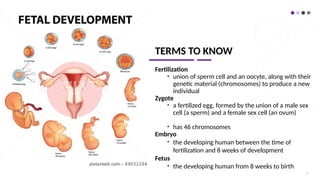
TERMS TO KNOW
Fertilization
•union of sperm cell and an oocyte, along with their
genetic material (chromosomes) to produce a new
individual
Zygote
• a fertilized egg, formed by the union of a male sex
cell (a sperm) and a female sex cell (an ovum)
• has 46 chromosomes
Embryo
• the developing human between the time of
fertilization and 8 weeks of development
Fetus
• the developing human from 8 weeks to birth
5
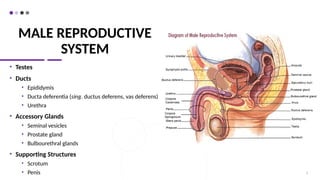
MALE REPRODUCTIVE
SYSTEM
• Scrotum
•A saclike structure containing the testes
• Divided into right and left internal compartments by an
incomplete connective tissue septum
• Beneath the scrotum skin are a layer of loose connective
tissue and a layer of smooth muscle called the DARTOS
MUSCLE
• Dartos and Cremaster muscles (extensions of abdominal
muscles into the scrotum) help regulate testes
temperature
7
8.
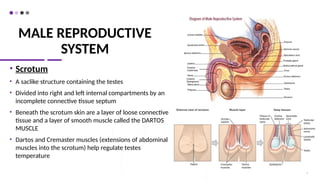
MALE REPRODUCTIVE
SYSTEM
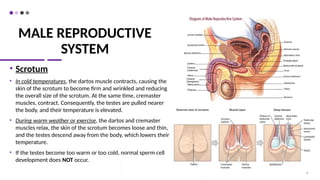
• Scrotum
•In cold temperatures, the dartos muscle contracts, causing the
skin of the scrotum to become firm and wrinkled and reducing
the overall size of the scrotum. At the same time, cremaster
muscles, contract. Consequently, the testes are pulled nearer
the body, and their temperature is elevated.
• During warm weather or exercise, the dartos and cremaster
muscles relax, the skin of the scrotum becomes loose and thin,
and the testes descend away from the body, which lowers their
temperature.
• If the testes become too warm or too cold, normal sperm cell
development does NOT occur.
8
9.
MALE REPRODUCTIVE
SYSTEM
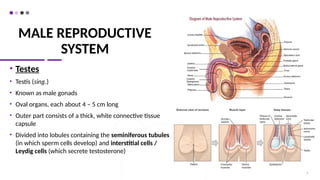
• Testes
•Testis (sing.)
• Known as male gonads
• Oval organs, each about 4 – 5 cm long
• Outer part consists of a thick, white connective tissue
capsule
• Divided into lobules containing the seminiferous tubules
(in which sperm cells develop) and interstitial cells /
Leydig cells (which secrete testosterone)
9
10.
MALE REPRODUCTIVE
SYSTEM
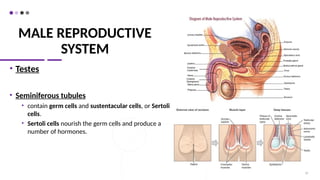
• Testes
•Seminiferous tubules
• contain germ cells and sustentacular cells, or Sertoli
cells.
• Sertoli cells nourish the germ cells and produce a
number of hormones.
10
11.
MALE REPRODUCTIVE
SYSTEM
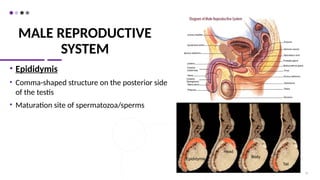
• Epididymis
•Comma-shaped structure on the posterior side
of the testis
• Maturation site of spermatozoa/sperms
11
Epididymis
Body
Head
Tail
12.
MALE REPRODUCTIVE
SYSTEM
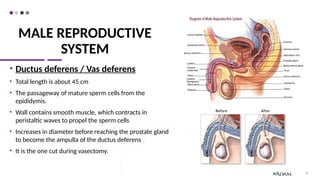
• Ductusdeferens / Vas deferens
• Total length is about 45 cm
• The passageway of mature sperm cells from the
epididymis.
• Wall contains smooth muscle, which contracts in
peristaltic waves to propel the sperm cells
• Increases in diameter before reaching the prostate gland
to become the ampulla of the ductus deferens
• It is the one cut during vasectomy.
12
13.
Why does onetesticle hang lower than the other?
•This condition assists in protecting the testicles from injury
by enabling them to glide one above the other when the
thigh are closely approximated and thus, to avoid
compression.
14.
MALE REPRODUCTIVE
SYSTEM
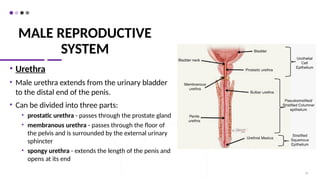
• Urethra
•Male urethra extends from the urinary bladder
to the distal end of the penis.
• Can be divided into three parts:
• prostatic urethra - passes through the prostate gland
• membranous urethra - passes through the floor of
the pelvis and is surrounded by the external urinary
sphincter
• spongy urethra - extends the length of the penis and
opens at its end
14
15.
MALE REPRODUCTIVE
SYSTEM
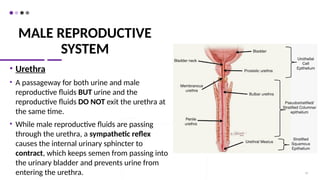
• Urethra
•A passageway for both urine and male
reproductive fluids BUT urine and the
reproductive fluids DO NOT exit the urethra at
the same time.
• While male reproductive fluids are passing
through the urethra, a sympathetic reflex
causes the internal urinary sphincter to
contract, which keeps semen from passing into
the urinary bladder and prevents urine from
entering the urethra. 15
16.
MALE REPRODUCTIVE
SYSTEM
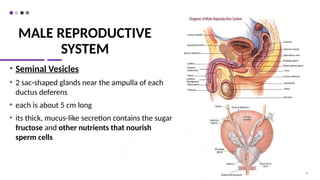
• SeminalVesicles
• 2 sac-shaped glands near the ampulla of each
ductus deferens
• each is about 5 cm long
• its thick, mucus-like secretion contains the sugar
fructose and other nutrients that nourish
sperm cells
16
17.
MALE REPRODUCTIVE
SYSTEM
• SeminalVesicles
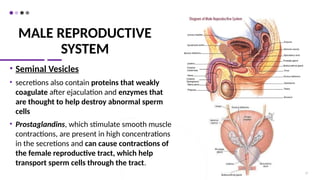
• secretions also contain proteins that weakly
coagulate after ejaculation and enzymes that
are thought to help destroy abnormal sperm
cells
• Prostaglandins, which stimulate smooth muscle
contractions, are present in high concentrations
in the secretions and can cause contractions of
the female reproductive tract, which help
transport sperm cells through the tract.
17
18.
MALE REPRODUCTIVE
SYSTEM
• ProstateGland
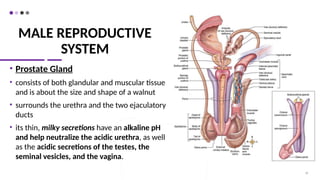
• consists of both glandular and muscular tissue
and is about the size and shape of a walnut
• surrounds the urethra and the two ejaculatory
ducts
• its thin, milky secretions have an alkaline pH
and help neutralize the acidic urethra, as well
as the acidic secretions of the testes, the
seminal vesicles, and the vagina.
18
19.
MALE REPRODUCTIVE
SYSTEM
• ProstateGland
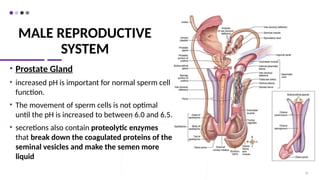
• increased pH is important for normal sperm cell
function.
• The movement of sperm cells is not optimal
until the pH is increased to between 6.0 and 6.5.
• secretions also contain proteolytic enzymes
that break down the coagulated proteins of the
seminal vesicles and make the semen more
liquid
19
20.
MALE REPRODUCTIVE
SYSTEM
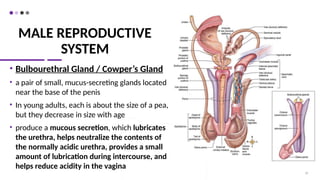
• BulbourethralGland / Cowper’s Gland
• a pair of small, mucus-secreting glands located
near the base of the penis
• In young adults, each is about the size of a pea,
but they decrease in size with age
• produce a mucous secretion, which lubricates
the urethra, helps neutralize the contents of
the normally acidic urethra, provides a small
amount of lubrication during intercourse, and
helps reduce acidity in the vagina
20
21.
MALE REPRODUCTIVE
SYSTEM
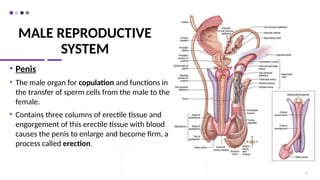
• Penis
•The male organ for copulation and functions in
the transfer of sperm cells from the male to the
female.
• Contains three columns of erectile tissue and
engorgement of this erectile tissue with blood
causes the penis to enlarge and become firm, a
process called erection.
21
22.
MALE REPRODUCTIVE
SYSTEM
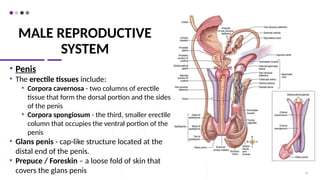
• Penis
•The erectile tissues include:
• Corpora cavernosa - two columns of erectile
tissue that form the dorsal portion and the sides
of the penis
• Corpora spongiosum - the third, smaller erectile
column that occupies the ventral portion of the
penis
• Glans penis - cap-like structure located at the
distal end of the penis.
• Prepuce / Foreskin – a loose fold of skin that
covers the glans penis 22
23.
MALE REPRODUCTIVE
SYSTEM
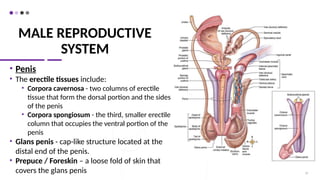
• Penis
•The erectile tissues include:
• Corpora cavernosa - two columns of erectile
tissue that form the dorsal portion and the sides
of the penis
• Corpora spongiosum - the third, smaller erectile
column that occupies the ventral portion of the
penis
• Glans penis - cap-like structure located at the
distal end of the penis.
• Prepuce / Foreskin – a loose fold of skin that
covers the glans penis 23
24.
Seminal Fluid /Semen
• A mixture of sperm cells and secretions from the male reproductive
glands
• Normal volume: 2–5 mL, with each mL of semen typically
containing about 100 million sperm cells.
• Four fractions:
• 60% - accounts for the secretions from the seminal vesicles
• 30% - accounts for the secretions from the prostate gland
• 5% - accounts for the secretions from the testes
• 5% - accounts for the secretions from the bulbourethral glands
25.
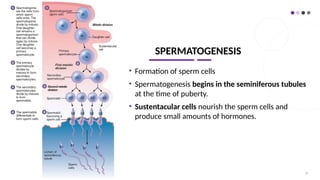
SPERMATOGENESIS
• Formation ofsperm cells
• Spermatogenesis begins in the seminiferous tubules
at the time of puberty.
• Sustentacular cells nourish the sperm cells and
produce small amounts of hormones.
25
26.
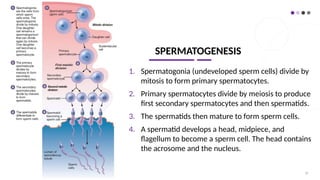
SPERMATOGENESIS
1. Spermatogonia (undevelopedsperm cells) divide by
mitosis to form primary spermatocytes.
2. Primary spermatocytes divide by meiosis to produce
first secondary spermatocytes and then spermatids.
3. The spermatids then mature to form sperm cells.
4. A spermatid develops a head, midpiece, and
flagellum to become a sperm cell. The head contains
the acrosome and the nucleus.
26
27.
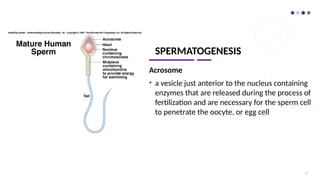
SPERMATOGENESIS
Acrosome
• a vesiclejust anterior to the nucleus containing
enzymes that are released during the process of
fertilization and are necessary for the sperm cell
to penetrate the oocyte, or egg cell
27
28.
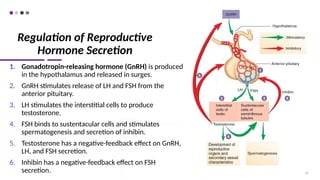
Regulation of Reproductive
HormoneSecretion
1. Gonadotropin-releasing hormone (GnRH) is produced
in the hypothalamus and released in surges.
2. GnRH stimulates release of LH and FSH from the
anterior pituitary.
3. LH stimulates the interstitial cells to produce
testosterone.
4. FSH binds to sustentacular cells and stimulates
spermatogenesis and secretion of inhibin.
5. Testosterone has a negative-feedback effect on GnRH,
LH, and FSH secretion.
6. Inhibin has a negative-feedback effect on FSH
secretion. 28
29.
Puberty in Males
•Puberty - sequence of events by which a child is
transformed into a young adult
• In boys, puberty commonly begins between the
ages of 12 and 14 and is largely completed by age
18.
• Before puberty, small amounts of testosterone,
secreted by the testes and the adrenal cortex,
inhibit GnRH release.
• During puberty, testosterone does not completely
suppress GnRH release, resulting in increased
production of FSH, LH, and testosterone.
29
30.
Effects of Testosterone
Testosterone– major male hormone
secreted by the testes
causes enlargement & differentiation
of the male genitals & the reproductive
duct system during puberty
necessary for spermatogenesis & for
the development of male secondary
sexual characteristics
30
31.
Effects of Testosterone
Secondarysexual characteristics:
• Those structural and behavioral changes,
other than in the reproductive organs, that
develop at puberty and distinguish males
from females.
• Include hair distribution and growth, skin
texture, fat distribution, skeletal muscle
growth, and changes in the larynx.
• After puberty, testosterone maintains the
adult structure of the male genitals,
reproductive ducts, and secondary sexual
characteristics.
31
32.
Male Sexual Behaviorand The Male Sex Act
•Testosterone - required for normal sex drive
•Male sex act - a complex series of reflexes that result in
erection of the penis, secretion of mucus into the urethra,
emission, and ejaculation
•Erection – the first major component of the male sex act
•Emission – the movement of sperm cells, mucus, prostatic
secretions, and seminal vesicle secretions into the
prostatic, membranous, and spongy urethra
33.
Male Sexual Behaviorand The Male Sex Act
•Ejaculation - the forceful expulsion of the secretions that
have accumulated in the urethra to the exterior
•Orgasm / Climax – an intense sensation, that result from
pleasurable sensations that occur during the male sex act
•Resolution – a phase that occurs after ejaculation. During
resolution, the penis becomes flaccid, an overall feeling of
satisfaction exists, and the male is unable to achieve
erection and a second ejaculation.
34.
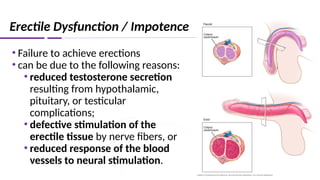
Erectile Dysfunction /Impotence
• Failure to achieve erections
• can be due to the following reasons:
• reduced testosterone secretion
resulting from hypothalamic,
pituitary, or testicular
complications;
• defective stimulation of the
erectile tissue by nerve fibers, or
• reduced response of the blood
vessels to neural stimulation.
35.
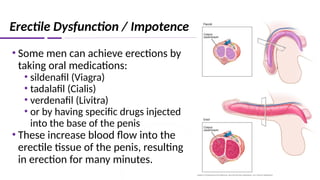
Erectile Dysfunction /Impotence
• Some men can achieve erections by
taking oral medications:
• sildenafil (Viagra)
• tadalafil (Cialis)
• verdenafil (Livitra)
• or by having specific drugs injected
into the base of the penis
• These increase blood flow into the
erectile tissue of the penis, resulting
in erection for many minutes.
36.
Infertility in Males
•Infertility - reduced or diminished fertility
• most common cause of infertility in males is a low sperm cell count
• If the sperm cell count drops to below 20 million sperm cells per mL, the male is
usually sterile.
• Decreased sperm cell count can be due to the following:
• damage to the testes as a result of trauma, radiation, cryptorchidism
• infections, such as mumps, which block the ducts in the epididymis
• inadequate secretion of LH and FSH, which can be caused by hypothyroidism,
trauma to the hypothalamus, infarctions of the hypothalamus or anterior
pituitary gland, or tumors
• decreased testosterone secretion
37.
Infertility in Males
•reduced fertility is possible if sperm cell structure is abnormal, due to
chromosomal abnormalities caused by genetic factors
• infertility can also be caused by reduced sperm cell motility
• A major cause of reduced sperm cell motility is the presence of
antisperm antibodies, which are produced by the immune system and
bind to sperm cells.
• In cases of infertility due to low sperm cell count or reduced motility,
fertility can sometimes be achieved by collecting several ejaculations,
concentrating the sperm cells, and inserting them into the female’s
reproductive tract, a process called artificial insemination.
•Specimen Collection:
• Abstainfrom sex or masturbation for a period of 3-5 days and not longer
than 7 days
• Prolonged abstinence will cause increased semen volume but decreased sperm motility.
• Always note the time of :
• Collection- usually done at room temperature but should be maintained at 370
C. If done outside,
semen must be transported in the laboratory within 1 hour.
• Liquefaction- sperm analysis should only be done after complete semen liquefaction. Normal
liquefaction time: 30-60 minutes. If complete liquefaction is not necessary:
• Break mucus and clumps
• Add chemicals like amylase or bromelin, plasmin & chymotrypsin
39
Seminal Fluid Analysis
40.
40
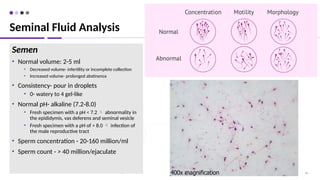
Semen
• Normal volume:2-5 ml
• Decreased volume- infertility or incomplete collection
• Increased volume- prolonged abstinence
• Consistency- pour in droplets
• 0- watery to 4 gel-like
• Normal pH- alkaline (7.2-8.0)
• Fresh specimen with a pH < 7.2 abnormality in
the epididymis, vas deferens and seminal vesicle
• Fresh specimen with a pH of > 8.0 infection of
the male reproductive tract
• Sperm concentration - 20-160 million/ml
• Sperm count - > 40 million/ejaculate
Seminal Fluid Analysis
41.
41
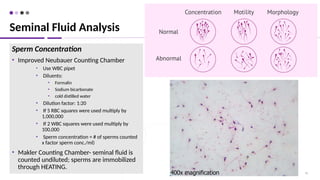
Sperm Concentration
• ImprovedNeubauer Counting Chamber
• Use WBC pipet
• Diluents:
• Formalin
• Sodium bicarbonate
• cold distilled water
• Dilution factor: 1:20
• If 5 RBC squares were used multiply by
1,000,000
• If 2 WBC squares were used multiply by
100,000
• Sperm concentration = # of sperms counted
x factor sperm conc./ml)
• Makler Counting Chamber- seminal fluid is
counted undiluted; sperms are immobilized
through HEATING.
Seminal Fluid Analysis
42.
42
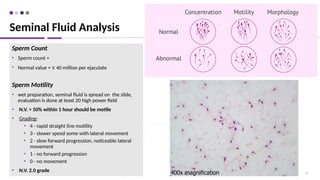
Sperm Count
• Spermcount =
• Normal value = ≥ 40 million per ejaculate
Sperm Motility
• wet preparation, seminal fluid is spread on the slide,
evaluation is done at least 20 high power field
• N.V. > 50% within 1 hour should be motile
• Grading:
• 4 - rapid straight line motility
• 3 - slower speed some with lateral movement
• 2 - slow forward progression, noticeable lateral
movement
• 1 - no forward progression
• 0 - no movement
• N.V. 2.0 grade
Seminal Fluid Analysis
43.
43
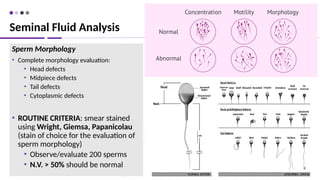
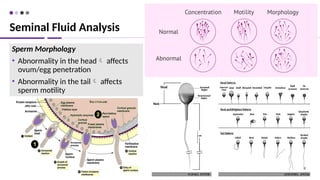
Sperm Morphology
• Completemorphology evaluation:
• Head defects
• Midpiece defects
• Tail defects
• Cytoplasmic defects
• ROUTINE CRITERIA: smear stained
using Wright, Giemsa, Papanicolau
(stain of choice for the evaluation of
sperm morphology)
• Observe/evaluate 200 sperms
• N.V. > 50% should be normal
Seminal Fluid Analysis
44.
44
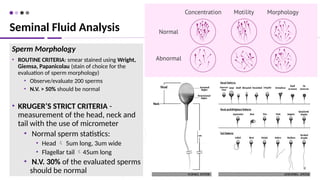
Sperm Morphology
• ROUTINECRITERIA: smear stained using Wright,
Giemsa, Papanicolau (stain of choice for the
evaluation of sperm morphology)
• Observe/evaluate 200 sperms
• N.V. > 50% should be normal
• KRUGER’S STRICT CRITERIA -
measurement of the head, neck and
tail with the use of micrometer
• Normal sperm statistics:
• Head 5um long, 3um wide
• Flagellar tail 45um long
• N.V. 30% of the evaluated sperms
should be normal
Seminal Fluid Analysis
45.
45
Sperm Morphology
• Abnormalityin the head affects
ovum/egg penetration
• Abnormality in the tail affects
sperm motility
Seminal Fluid Analysis
46.
46
• Sexual activityis often maintained in men as they age, but the
frequency of sexual intercourse usually decreases gradually.
• Benign prostatic enlargement is common after 50 years of age. A
major consequence of prostatic enlargement is blockage of the
prostatic urethra.
• The frequency of prostate cancer also increases as men age and is
a significant cause of death in men.
• The tendency for erectile dysfunction increases as men age.
Effects of Aging on Male Reproductive System
47.
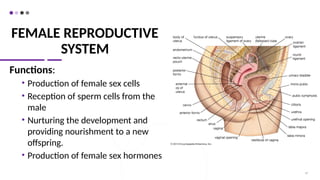
FEMALE REPRODUCTIVE
SYSTEM
Functions:
• Productionof female sex cells
• Reception of sperm cells from the
male
• Nurturing the development and
providing nourishment to a new
offspring.
• Production of female sex hormones
47
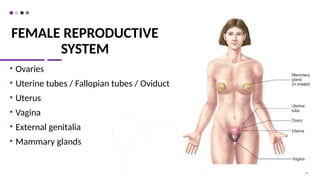
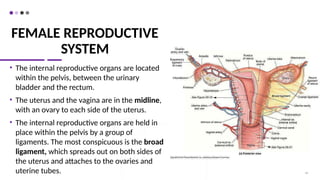
FEMALE REPRODUCTIVE
SYSTEM
• Theinternal reproductive organs are located
within the pelvis, between the urinary
bladder and the rectum.
• The uterus and the vagina are in the midline,
with an ovary to each side of the uterus.
• The internal reproductive organs are held in
place within the pelvis by a group of
ligaments. The most conspicuous is the broad
ligament, which spreads out on both sides of
the uterus and attaches to the ovaries and
uterine tubes. 49
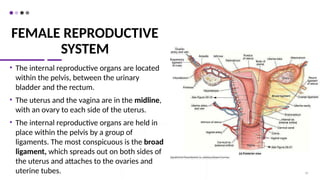
50.
FEMALE REPRODUCTIVE
SYSTEM
• Theinternal reproductive organs are located
within the pelvis, between the urinary
bladder and the rectum.
• The uterus and the vagina are in the midline,
with an ovary to each side of the uterus.
• The internal reproductive organs are held in
place within the pelvis by a group of
ligaments. The most conspicuous is the broad
ligament, which spreads out on both sides of
the uterus and attaches to the ovaries and
uterine tubes. 50
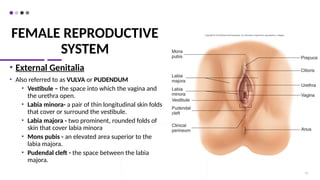
51.
FEMALE REPRODUCTIVE
SYSTEM
• ExternalGenitalia
• Also referred to as VULVA or PUDENDUM
• Vestibule – the space into which the vagina and
the urethra open.
• Labia minora- a pair of thin longitudinal skin folds
that cover or surround the vestibule.
• Labia majora - two prominent, rounded folds of
skin that cover labia minora
• Mons pubis - an elevated area superior to the
labia majora.
• Pudendal cleft - the space between the labia
majora.
51
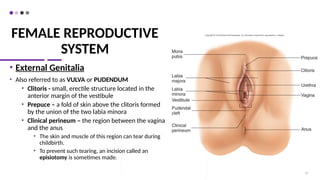
52.
FEMALE REPRODUCTIVE
SYSTEM
• ExternalGenitalia
• Also referred to as VULVA or PUDENDUM
• Clitoris - small, erectile structure located in the
anterior margin of the vestibule
• Prepuce – a fold of skin above the clitoris formed
by the union of the two labia minora
• Clinical perineum – the region between the vagina
and the anus
• The skin and muscle of this region can tear during
childbirth.
• To prevent such tearing, an incision called an
episiotomy is sometimes made.
52
53.
FEMALE REPRODUCTIVE
SYSTEM
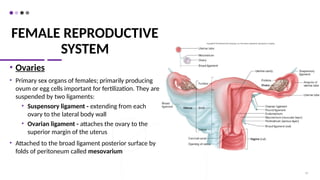
• Ovaries
•Primary sex organs of females; primarily producing
ovum or egg cells important for fertilization. They are
suspended by two ligaments:
• Suspensory ligament - extending from each
ovary to the lateral body wall
• Ovarian ligament - attaches the ovary to the
superior margin of the uterus
• Attached to the broad ligament posterior surface by
folds of peritoneum called mesovarium
53
54.
FEMALE REPRODUCTIVE
SYSTEM
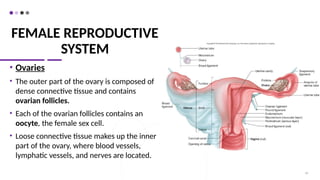
• Ovaries
•The outer part of the ovary is composed of
dense connective tissue and contains
ovarian follicles.
• Each of the ovarian follicles contains an
oocyte, the female sex cell.
• Loose connective tissue makes up the inner
part of the ovary, where blood vessels,
lymphatic vessels, and nerves are located.
54
55.
FEMALE REPRODUCTIVE
SYSTEM
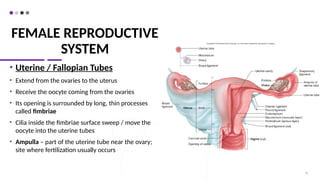
• Uterine/ Fallopian Tubes
• Extend from the ovaries to the uterus
• Receive the oocyte coming from the ovaries
• Its opening is surrounded by long, thin processes
called fimbriae
• Cilia inside the fimbriae surface sweep / move the
oocyte into the uterine tubes
• Ampulla – part of the uterine tube near the ovary;
site where fertilization usually occurs
55
56.
FEMALE REPRODUCTIVE
SYSTEM
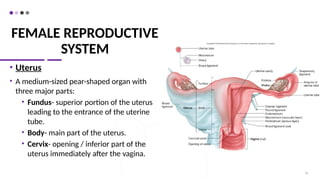
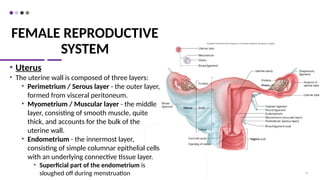
• Uterus
•A medium-sized pear-shaped organ with
three major parts:
• Fundus- superior portion of the uterus
leading to the entrance of the uterine
tube.
• Body- main part of the uterus.
• Cervix- opening / inferior part of the
uterus immediately after the vagina.
56
57.
FEMALE REPRODUCTIVE
SYSTEM
• Uterus
•The uterine wall is composed of three layers:
• Perimetrium / Serous layer - the outer layer,
formed from visceral peritoneum.
• Myometrium / Muscular layer - the middle
layer, consisting of smooth muscle, quite
thick, and accounts for the bulk of the
uterine wall.
• Endometrium - the innermost layer,
consisting of simple columnar epithelial cells
with an underlying connective tissue layer.
• Superficial part of the endometrium is
sloughed off during menstruation 57
58.
FEMALE REPRODUCTIVE
SYSTEM
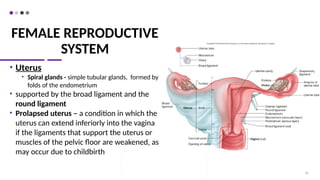
• Uterus
•Spiral glands - simple tubular glands, formed by
folds of the endometrium
• supported by the broad ligament and the
round ligament
• Prolapsed uterus – a condition in which the
uterus can extend inferiorly into the vagina
if the ligaments that support the uterus or
muscles of the pelvic floor are weakened, as
may occur due to childbirth
58
59.
FEMALE REPRODUCTIVE
SYSTEM
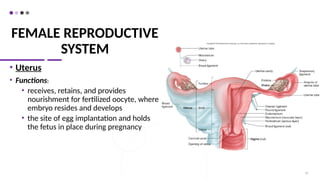
• Uterus
•Functions:
• receives, retains, and provides
nourishment for fertilized oocyte, where
embryo resides and develops
• the site of egg implantation and holds
the fetus in place during pregnancy
59
60.
FEMALE REPRODUCTIVE
SYSTEM
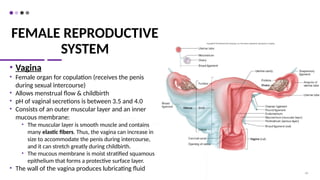
• Vagina
•Female organ for copulation (receives the penis
during sexual intercourse)
• Allows menstrual flow & childbirth
• pH of vaginal secretions is between 3.5 and 4.0
• Consists of an outer muscular layer and an inner
mucous membrane:
• The muscular layer is smooth muscle and contains
many elastic fibers. Thus, the vagina can increase in
size to accommodate the penis during intercourse,
and it can stretch greatly during childbirth.
• The mucous membrane is moist stratified squamous
epithelium that forms a protective surface layer.
• The wall of the vagina produces lubricating fluid
60
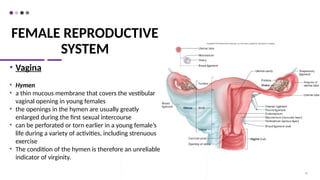
61.
FEMALE REPRODUCTIVE
SYSTEM
• Vagina
•Hymen
• a thin mucous membrane that covers the vestibular
vaginal opening in young females
• the openings in the hymen are usually greatly
enlarged during the first sexual intercourse
• can be perforated or torn earlier in a young female’s
life during a variety of activities, including strenuous
exercise
• The condition of the hymen is therefore an unreliable
indicator of virginity.
61
62.
FEMALE REPRODUCTIVE
SYSTEM
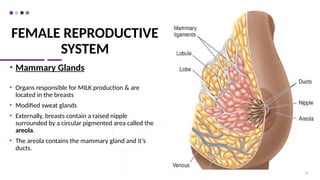
• MammaryGlands
• Organs responsible for MILK production & are
located in the breasts
• Modified sweat glands
• Externally, breasts contain a raised nipple
surrounded by a circular pigmented area called the
areola.
• The areola contains the mammary gland and it’s
ducts.
62
63.
FEMALE REPRODUCTIVE
SYSTEM
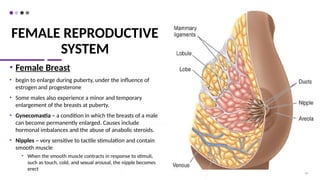
• FemaleBreast
• begin to enlarge during puberty, under the influence of
estrogen and progesterone
• Some males also experience a minor and temporary
enlargement of the breasts at puberty.
• Gynecomastia – a condition in which the breasts of a male
can become permanently enlarged. Causes include
hormonal imbalances and the abuse of anabolic steroids.
• Nipples – very sensitive to tactile stimulation and contain
smooth muscle
• When the smooth muscle contracts in response to stimuli,
such as touch, cold, and sexual arousal, the nipple becomes
erect
63
64.
OOGENESIS, FOLLICLE
DEVELOPMENT, ANDFERTILIZATION
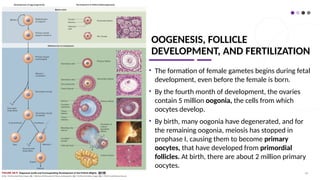
• The formation of female gametes begins during fetal
development, even before the female is born.
• By the fourth month of development, the ovaries
contain 5 million oogonia, the cells from which
oocytes develop.
• By birth, many oogonia have degenerated, and for
the remaining oogonia, meiosis has stopped in
prophase I, causing them to become primary
oocytes, that have developed from primordial
follicles. At birth, there are about 2 million primary
oocytes.
64
65.
OOGENESIS, FOLLICLE
DEVELOPMENT, ANDFERTILIZATION
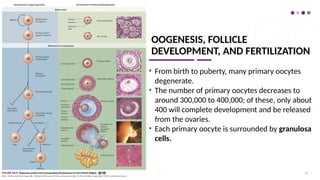
• From birth to puberty, many primary oocytes
degenerate.
• The number of primary oocytes decreases to
around 300,000 to 400,000; of these, only about
400 will complete development and be released
from the ovaries.
• Each primary oocyte is surrounded by granulosa
cells.
65
66.
OOGENESIS, FOLLICLE
DEVELOPMENT, ANDFERTILIZATION
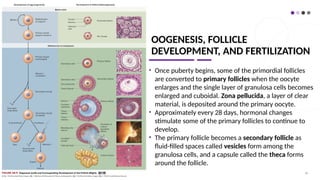
• Once puberty begins, some of the primordial follicles
are converted to primary follicles when the oocyte
enlarges and the single layer of granulosa cells becomes
enlarged and cuboidal. Zona pellucida, a layer of clear
material, is deposited around the primary oocyte.
• Approximately every 28 days, hormonal changes
stimulate some of the primary follicles to continue to
develop.
• The primary follicle becomes a secondary follicle as
fluid-filled spaces called vesicles form among the
granulosa cells, and a capsule called the theca forms
around the follicle.
66
67.
OOGENESIS, FOLLICLE
DEVELOPMENT, ANDFERTILIZATION
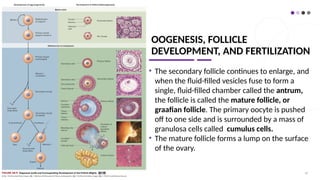
• The secondary follicle continues to enlarge, and
when the fluid-filled vesicles fuse to form a
single, fluid-filled chamber called the antrum,
the follicle is called the mature follicle, or
graafian follicle. The primary oocyte is pushed
off to one side and is surrounded by a mass of
granulosa cells called cumulus cells.
• The mature follicle forms a lump on the surface
of the ovary.
67
68.
OOGENESIS, FOLLICLE
DEVELOPMENT, ANDFERTILIZATION
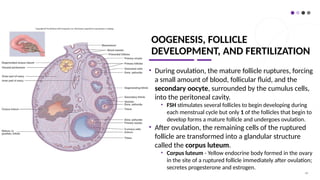
• During ovulation, the mature follicle ruptures, forcing
a small amount of blood, follicular fluid, and the
secondary oocyte, surrounded by the cumulus cells,
into the peritoneal cavity.
• FSH stimulates several follicles to begin developing during
each menstrual cycle but only 1 of the follicles that begin to
develop forms a mature follicle and undergoes ovulation.
• After ovulation, the remaining cells of the ruptured
follicle are transformed into a glandular structure
called the corpus luteum.
• Corpus luteum - Yellow endocrine body formed in the ovary
in the site of a ruptured follicle immediately after ovulation;
secretes progesterone and estrogen.
68
69.
OOGENESIS, FOLLICLE
DEVELOPMENT, ANDFERTILIZATION
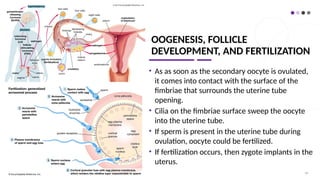
• As as soon as the secondary oocyte is ovulated,
it comes into contact with the surface of the
fimbriae that surrounds the uterine tube
opening.
• Cilia on the fimbriae surface sweep the oocyte
into the uterine tube.
• If sperm is present in the uterine tube during
ovulation, oocyte could be fertilized.
• If fertilization occurs, then zygote implants in the
uterus.
69
70.
OOGENESIS, FOLLICLE
DEVELOPMENT, ANDFERTILIZATION
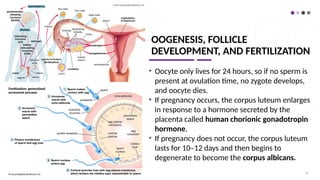
• Oocyte only lives for 24 hours, so if no sperm is
present at ovulation time, no zygote develops,
and oocyte dies.
• If pregnancy occurs, the corpus luteum enlarges
in response to a hormone secreted by the
placenta called human chorionic gonadotropin
hormone.
• If pregnancy does not occur, the corpus luteum
lasts for 10–12 days and then begins to
degenerate to become the corpus albicans.
70
71.
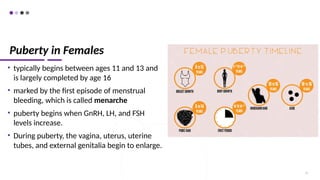
Puberty in Females
•typically begins between ages 11 and 13 and
is largely completed by age 16
• marked by the first episode of menstrual
bleeding, which is called menarche
• puberty begins when GnRH, LH, and FSH
levels increase.
• During puberty, the vagina, uterus, uterine
tubes, and external genitalia begin to enlarge.
71
72.
Puberty in Females
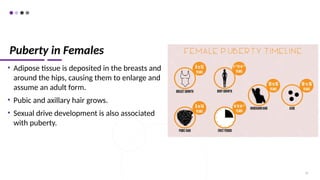
•Adipose tissue is deposited in the breasts and
around the hips, causing them to enlarge and
assume an adult form.
• Pubic and axillary hair grows.
• Sexual drive development is also associated
with puberty.
72
73.
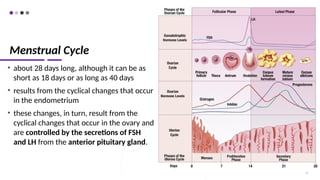
Menstrual Cycle
• about28 days long, although it can be as
short as 18 days or as long as 40 days
• results from the cyclical changes that occur
in the endometrium
• these changes, in turn, result from the
cyclical changes that occur in the ovary and
are controlled by the secretions of FSH
and LH from the anterior pituitary gland.
73
74.
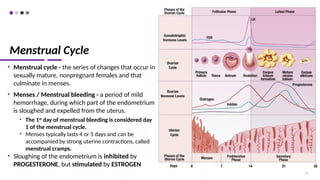
Menstrual Cycle
• Menstrualcycle - the series of changes that occur in
sexually mature, nonpregnant females and that
culminate in menses.
• Menses / Menstrual bleeding - a period of mild
hemorrhage, during which part of the endometrium
is sloughed and expelled from the uterus.
• The 1st
day of menstrual bleeding is considered day
1 of the menstrual cycle.
• Menses typically lasts 4 or 5 days and can be
accompanied by strong uterine contractions, called
menstrual cramps.
• Sloughing of the endometrium is inhibited by
PROGESTERONE, but stimulated by ESTROGEN
74
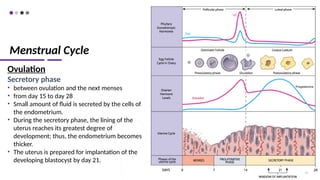
75.
Menstrual Cycle
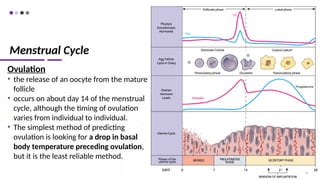
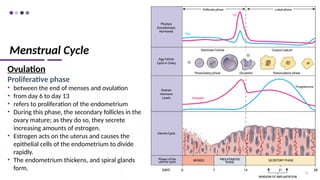
Ovulation
• therelease of an oocyte from the mature
follicle
• occurs on about day 14 of the menstrual
cycle, although the timing of ovulation
varies from individual to individual.
• The simplest method of predicting
ovulation is looking for a drop in basal
body temperature preceding ovulation,
but it is the least reliable method.
75
76.
Menstrual Cycle
Ovulation
Proliferative phase
•between the end of menses and ovulation
• from day 6 to day 13
• refers to proliferation of the endometrium
• During this phase, the secondary follicles in the
ovary mature; as they do so, they secrete
increasing amounts of estrogen.
• Estrogen acts on the uterus and causes the
epithelial cells of the endometrium to divide
rapidly.
• The endometrium thickens, and spiral glands
form.
76
77.
Menstrual Cycle
Ovulation
Secretory phase
•between ovulation and the next menses
• from day 15 to day 28
• Small amount of fluid is secreted by the cells of
the endometrium.
• During the secretory phase, the lining of the
uterus reaches its greatest degree of
development; thus, the endometrium becomes
thicker.
• The uterus is prepared for implantation of the
developing blastocyst by day 21.
77
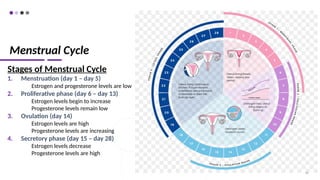
78.
Menstrual Cycle
Stages ofMenstrual Cycle
1. Menstruation (day 1 – day 5)
Estrogen and progesterone levels are low
2. Proliferative phase (day 6 – day 13)
Estrogen levels begin to increase
Progesterone levels remain low
3. Ovulation (day 14)
Estrogen levels are high
Progesterone levels are increasing
4. Secretory phase (day 15 – day 28)
Estrogen levels decrease
Progesterone levels are high
78
79.
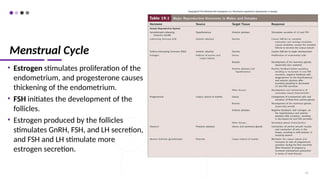
Menstrual Cycle
• Estrogenstimulates proliferation of the
endometrium, and progesterone causes
thickening of the endometrium.
• FSH initiates the development of the
follicles.
• Estrogen produced by the follicles
stimulates GnRH, FSH, and LH secretion,
and FSH and LH stimulate more
estrogen secretion.
79
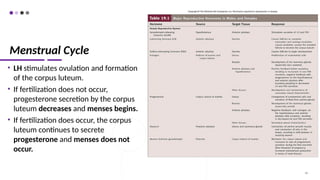
80.
Menstrual Cycle
• LHstimulates ovulation and formation
of the corpus luteum.
• If fertilization does not occur,
progesterone secretion by the corpus
luteum decreases and menses begins.
• If fertilization does occur, the corpus
luteum continues to secrete
progesterone and menses does not
occur.
80
81.
Menstrual Cramps
• theresult of forceful myometrial
contractions that occur before and during
menstruation
• can result from excessive secretion of
prostaglandins
• As the endometrium of the uterus sloughs
off, it becomes inflamed, and prostaglandins
are produced as part of the inflammation.
• painful cramps can be alleviated by taking
medications, such as aspirin-like drugs, that
inhibit prostaglandin biosynthesis just
before the onset of menstruation.
82.
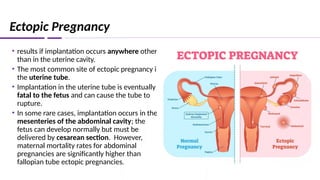
Ectopic Pregnancy
• resultsif implantation occurs anywhere other
than in the uterine cavity.
• The most common site of ectopic pregnancy is
the uterine tube.
• Implantation in the uterine tube is eventually
fatal to the fetus and can cause the tube to
rupture.
• In some rare cases, implantation occurs in the
mesenteries of the abdominal cavity; the
fetus can develop normally but must be
delivered by cesarean section. However,
maternal mortality rates for abdominal
pregnancies are significantly higher than
fallopian tube ectopic pregnancies.
83.
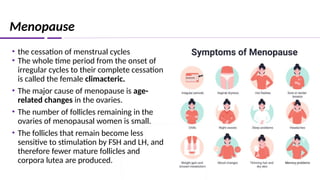
Menopause
• the cessationof menstrual cycles
• The whole time period from the onset of
irregular cycles to their complete cessation
is called the female climacteric.
• The major cause of menopause is age-
related changes in the ovaries.
• The number of follicles remaining in the
ovaries of menopausal women is small.
• The follicles that remain become less
sensitive to stimulation by FSH and LH, and
therefore fewer mature follicles and
corpora lutea are produced.
84.
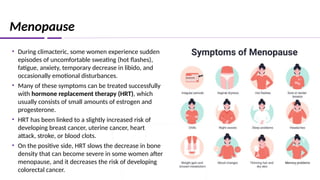
Menopause
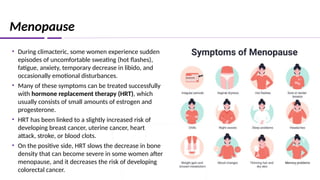
• During climacteric,some women experience sudden
episodes of uncomfortable sweating (hot flashes),
fatigue, anxiety, temporary decrease in libido, and
occasionally emotional disturbances.
• Many of these symptoms can be treated successfully
with hormone replacement therapy (HRT), which
usually consists of small amounts of estrogen and
progesterone.
• HRT has been linked to a slightly increased risk of
developing breast cancer, uterine cancer, heart
attack, stroke, or blood clots.
• On the positive side, HRT slows the decrease in bone
density that can become severe in some women after
menopause, and it decreases the risk of developing
colorectal cancer.
85.
Menopause
• During climacteric,some women experience sudden
episodes of uncomfortable sweating (hot flashes),
fatigue, anxiety, temporary decrease in libido, and
occasionally emotional disturbances.
• Many of these symptoms can be treated successfully
with hormone replacement therapy (HRT), which
usually consists of small amounts of estrogen and
progesterone.
• HRT has been linked to a slightly increased risk of
developing breast cancer, uterine cancer, heart
attack, stroke, or blood clots.
• On the positive side, HRT slows the decrease in bone
density that can become severe in some women after
menopause, and it decreases the risk of developing
colorectal cancer.
86.
Female Sexual Behaviorand The Female Sex Act
• Female sex drive is partially influenced by testosterone-like hormones
produced by the adrenal cortex and estrogen produced by the ovary.
• Autonomic nerves cause erectile tissue within the clitoris and around
the vaginal opening to become engorged with blood, the vestibular
glands to secrete mucus, and the vagina to produce a lubricating fluid.
• These secretions provide lubrication to allow easy entry and
movement of the penis in the vagina during intercourse.
87.
Female Sexual Behaviorand The Female Sex Act
•Tactile stimulation of the female’s genitals during sexual
intercourse and psychological stimuli normally trigger an
orgasm or climax.
•After the sex act, there is a period of resolution, which is
characterized by an overall sense of satisfaction and
relaxation.
•Females can experience successive orgasms.
•Orgasm is not necessary for fertilization to occur.
88.
Infertility in Females
CAUSES:
1.Malfunctions of the uterine tubes
• Occur when infections result in pelvic inflammatory disease (PID), which causes adhesions to
form in one or both of the uterine tubes.
2. Reduced hormone secretion from the pituitary gland or the ovaries
• Inadequate secretion of LH and FSH can occur for a variety of reasons, including
hypothyroidism or a tumor in or trauma to the hypothalamus or anterior pituitary.
• Decreased secretion of LH and FSH interrupts ovulation.
3. Interruption of implantation
• Can result from uterine tumors or conditions causing abnormal ovarian hormone secretion.
89.
89
• Menopause isthe most common age-related change in females.
• By age 50, the amount of estrogen and progesterone produced by the
ovaries has decreased.
• The uterus decreases in size, and the endometrium decreases in thickness.
• The times between menses become irregular and longer until menstruation
stops.
• The vaginal wall becomes thinner and less elastic, and there is less lubricant
in the vagina, resulting in an increased tendency for vaginal yeast infections
• Cancers of the breast, the cervix, and the ovaries increase in elderly women.
Effects of Aging on Female Reproductive System
90.
90
The following slidesinclude materials or images
regarding reproductive system disorders
that maybe disturbing to audiences.
Please be advised.
WARNING
91.
91
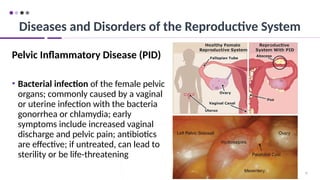
Pelvic Inflammatory Disease(PID)
• Bacterial infection of the female pelvic
organs; commonly caused by a vaginal
or uterine infection with the bacteria
gonorrhea or chlamydia; early
symptoms include increased vaginal
discharge and pelvic pain; antibiotics
are effective; if untreated, can lead to
sterility or be life-threatening
Diseases and Disorders of the Reproductive System
92.
92
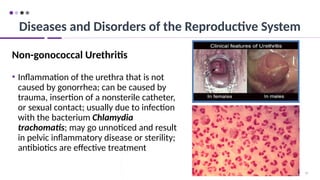
Non-gonococcal Urethritis
• Inflammationof the urethra that is not
caused by gonorrhea; can be caused by
trauma, insertion of a nonsterile catheter,
or sexual contact; usually due to infection
with the bacterium Chlamydia
trachomatis; may go unnoticed and result
in pelvic inflammatory disease or sterility;
antibiotics are effective treatment
Diseases and Disorders of the Reproductive System
93.
93
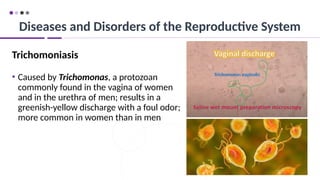
Trichomoniasis
• Caused byTrichomonas, a protozoan
commonly found in the vagina of women
and in the urethra of men; results in a
greenish-yellow discharge with a foul odor;
more common in women than in men
Diseases and Disorders of the Reproductive System
94.
94
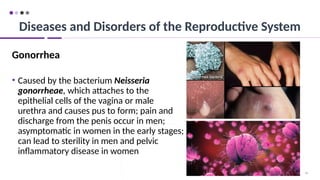
Gonorrhea
• Caused bythe bacterium Neisseria
gonorrheae, which attaches to the
epithelial cells of the vagina or male
urethra and causes pus to form; pain and
discharge from the penis occur in men;
asymptomatic in women in the early stages;
can lead to sterility in men and pelvic
inflammatory disease in women
Diseases and Disorders of the Reproductive System
95.
95
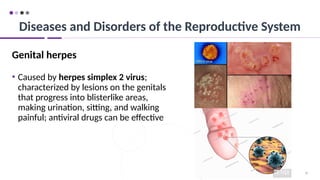
Genital herpes
• Causedby herpes simplex 2 virus;
characterized by lesions on the genitals
that progress into blisterlike areas,
making urination, sitting, and walking
painful; antiviral drugs can be effective
Diseases and Disorders of the Reproductive System
96.
96
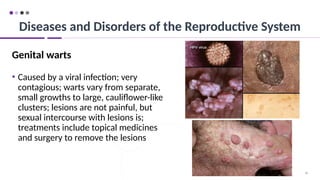
Genital warts
• Causedby a viral infection; very
contagious; warts vary from separate,
small growths to large, cauliflower-like
clusters; lesions are not painful, but
sexual intercourse with lesions is;
treatments include topical medicines
and surgery to remove the lesions
Diseases and Disorders of the Reproductive System
97.
97
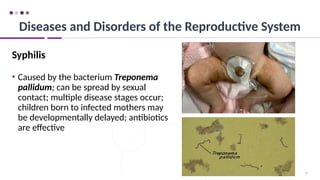
Syphilis
• Caused bythe bacterium Treponema
pallidum; can be spread by sexual
contact; multiple disease stages occur;
children born to infected mothers may
be developmentally delayed; antibiotics
are effective
Diseases and Disorders of the Reproductive System
98.
98
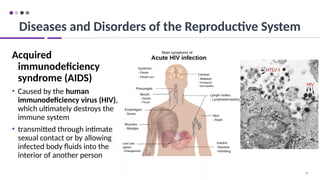
Acquired
immunodeficiency
syndrome (AIDS)
• Causedby the human
immunodeficiency virus (HIV),
which ultimately destroys the
immune system
• transmitted through intimate
sexual contact or by allowing
infected body fluids into the
interior of another person
Diseases and Disorders of the Reproductive System