Download to read offline

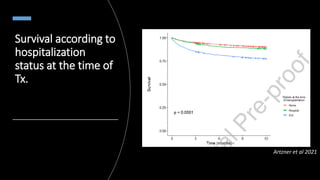

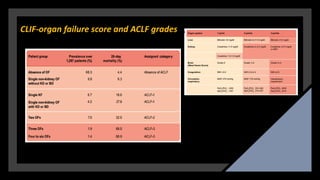

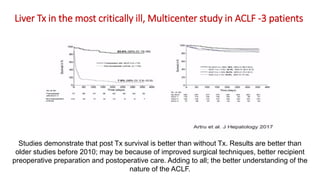
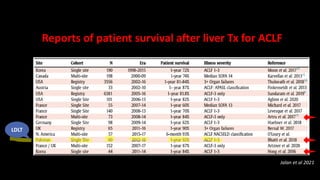

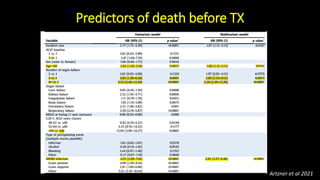
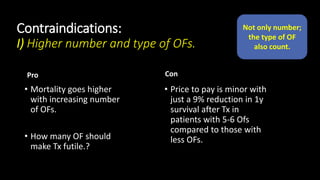
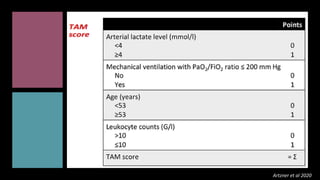
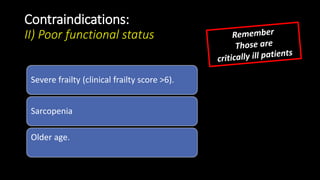

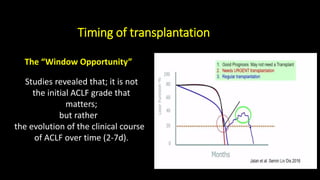





The document discusses liver transplantation for critically ill patients. It provides an agenda on the topic and discusses evidence that transplantation can provide a survival benefit for these patients. It examines different scores used to measure illness severity and transplant futility, such as MELD, CLIF-C ACLF, and organ failure scores. Contraindications for transplantation like number of organ failures, infections, and poor functional status are presented. Timing of transplantation is also important, with a window of opportunity for patients with evolving ACLF. Management of coagulopathy, fluids, and circulation in critically ill transplant candidates is covered. The conclusion is that transplantation can improve survival for ACLF patients when done promptly based on illness scores and the patient's clinical condition



































































