
Recommended
More Related Content
Similar to The contribution of spirituality and spiritual copingto anxi.docx
Similar to The contribution of spirituality and spiritual copingto anxi.docx (20)
More from rtodd643
More from rtodd643 (20)
Recently uploaded
Recently uploaded (20)
The contribution of spirituality and spiritual copingto anxi.docx
- 1. The contribution of spirituality and spiritual coping to anxiety and depression in women with a recent diagnosis of gynecological cancer N. BOSCAGLIA*, D.M. CLARKE*, T.W. JOBLINGy & M.A. QUINNz *Department of Psychological Medicine and General Practice, Monash University, Melbourne, Australia; yDepartment of Obstetrics and Gynaecology, Monash Medical Centre, Melbourne, Australia; and zDepartment of Obstetrics and Gynaecology, and Oncology Unit, Melbourne University, Royal Women’s Hospital, Melbourne, Australia Abstract. Boscaglia N, Clarke DM, Jobling TW, Quinn MA. The con- tribution of spirituality and spiritual coping to anxiety and depression in women with a recent diagnosis of gynecological cancer. Int J Gynecol Cancer 2005;15:755–761. The objective of this study was to determine whether, after accounting for illness and demographic variables, spiritual involvement and beliefs and positive and negative spiritual coping could account for any of the variation in anxiety and depression among women within 1 year’s diag-
- 2. nosis of gynecological cancer (GC). One hundred patients from out- patient GC clinics at two Melbourne-based hospitals completed a brief structured interview and self-report measures of anxiety, depression, spirituality, and spiritual coping. Using two sequential regression analy- ses, we found that younger women with more advanced disease, who used more negative spiritual coping, had a greater tendency towards depression and that the use of negative spiritual coping was associated with greater anxiety scores. Although not statistically significant, pa- tients with lower levels of generalized spirituality also tended to be more depressed. The site of disease and phase of treatment were not predictive of either anxiety or depression. We conclude that spirituality and spiritual coping are important to women with GC and that health professionals in the area should consider these issues. KEYWORDS: anxiety, coping, depression, gynecological
- 3. cancer, spirituality. In a recent issue of this journal, Ramondetta and Sills(1) published a review of the literature concerning the role of spirituality in gynecological cancer (GC). The authors concluded that ‘‘concerns for the spiritual health of patients may prove significant for both a patient’s comprehensive sense of well-being and for the relationship that is created between patients and physicians.’’ In this study, we examined empirically the relationship between spirituality and mood (ie, anxiety and depression). A diagnosis of cancer is a significant life event that may have considerable psychological, physical, and financial sequelae. In particular, a diagnosis of GC Address correspondence and reprint requests to: Nadia Boscaglia, Department of Psychological Medicine, Monash University, Monash Medical Centre, 246 Clayton Rd., Clayton, Victoria 3800, Australia. Email: [email protected] # 2005 IGCS Int J Gynecol Cancer 2005, 15, 755–761 may elicit disturbances to body image; feelings of helplessness, dependency, shame, guilt, and vulnera- bility; a sense of loss of femininity and motherhood; and sexual difficulties(1,2). Not surprisingly, women with GC have a heightened frequency of depression, anxiety, and adjustment disorders(3).
- 4. Certain factors that increase the risk for mood distur- bance among women with GC include site of cancer (ovarian cancer worst)(4,5), treatment with triple-agent chemotherapy, younger age(6,7), and current treat- ment(6,8). In general, more advanced cancers are associ- ated with more frequent psychiatric complications(9). Psychological health is important when faced with a diagnosis of cancer. Depressive symptoms in associa- tion with medical illness have been found to affect qual- ity of life and social functioning, exert a negative impact on treatment compliance(10), and lead to increased use of healthcare services(11). Similarly, anxiety can interfere with physical and psychosocial functioning; thus, for those who are physically compromised by illness, high levels of anxiety are of concern(12). Recent research indicates that spirituality is one factor that may contribute to good mental health during the course of cancer. Spirituality is a set of beliefs and atti- tudes that give meaning and purpose to life through a sense of connectedness with the self, others, the natu- ral environment, a higher power, and/or other super- natural forces. These beliefs and attitudes empower and transcend the self and are embodied in feelings, thoughts, experiences, and behaviors(13–15). Spirituality is a broader concept than religion or religiosity, which refers to organized beliefs and practices such as those found in formal denominations or recognized systems of theological ideas; as such, religion can be viewed as a dimension of spirituality(14,16). Among those with life-threatening illnesses, spirituality has been found to be positively associated with psychosocial adjust- ment(17) and quality of life(18); and spiritual well-being was inversely associated with death distress(19) and
- 5. anxiety(20). Religion and spirituality may be incorporated as part of one’s coping(21,22), whereby coping is defined as the process by which individuals respond to stress- ful stimuli. Within the coping process, there are two subprocesses, appraisal and coping efforts (or meth- ods). Appraisal refers to the individual’s evaluation of the event(23); this evaluation influences one’s coping efforts. Coping efforts are the actions through which coping can resolve the stressful event and has effects on physical and emotional health(24). Research shows that an individual’s mood and quality of life after receiving a cancer diagnosis can be, in part, accounted for by his/her coping efforts(25–27). People bring with them a general orienting system to the coping process. A spiritual orientation (eg, general beliefs, practices, aspirations, and relation- ships) is but one part of a larger orienting system(22). In the coping process, both the spiritual (general reli- gious and spiritual beliefs, involvement, and practi- ces) and nonspiritual elements of this orienting system are translated into specific methods of coping. It is these coping methods that have the most direct implications for health and well-being(14,28–30). In- deed, research indicates that specific spiritual coping efforts are better predictors of event outcomes (eg, mood, adjustment) than are measures of generalized spirituality(21,28,31). Put simply, spiritual coping is the use of religious/spiritual beliefs and practices to reduce the emotional distress caused by loss or change(32). Researchers(30) have identified two patterns of spiri- tual coping* (broadly termed, positive and negative)
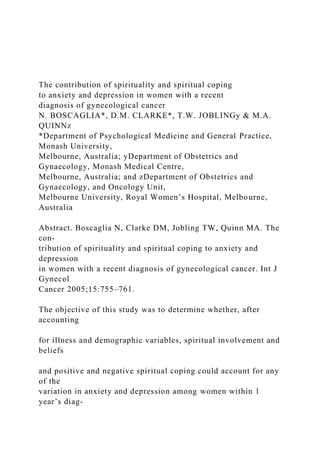
- 6. that have important implications for health. Positive spiritual coping methods reflect an expression of ‘‘a sense of spirituality, a secure relationship with God, a belief that there is meaning to be found in life, and a sense of spiritual connectedness with others’’(30, p712). In contrast, the negative spiritual coping pattern is an expression of ‘‘a less secure relationship with God, a tenuous and ominous view of the world, and a reli- gious struggle in the search for significance’’(30, p712). Each of the two patterns is made up of specific types of spiritual coping methods (Table 1). Research dem- onstrates that among various samples, the positive spiritual coping pattern was associated with fewer symptoms of psychological distress(30,33) and higher levels of stress-related growth(30); and the negative spiritual coping pattern was associated with more depression(30,33) and poor quality of life(30). There are few studies that have examined the impact of spirituality on psychological state in women with GC(1). This is surprising, given that there are sev- eral factors that make salient the study of spirituality in this particular group. Life-threatening events such as cancer, particularly those that pose threats to self- image or important areas of personal functioning, often lead to people relying on their spiritual re- sources(14,18). Further, religious and spiritual coping appears to be used more often by women than men(17). In this study, our aim was to determine *While Pargament et al.(28–30) use the term ‘‘religious coping,’’ we prefer the term ‘‘spiritual coping.’’ This difference in terminology is reflective of each author’s definition of the terms religion and spir-
- 7. ituality, that is, Pargament et al. view religion in much the same was as we view spirituality. 756 N. Boscaglia et al. # 2005 IGCS, International Journal of Gynecological Cancer 15, 755–761 whether spiritual involvement and beliefs and posi- tive and negative spiritual coping accounted for any of the variance in psychological distress (anxiety and depression) among women with GC, over and above that accounted for by illness and demographic variables. Materials and methods One hundred and twenty-three patients were re- cruited from outpatient GC clinics at the Royal Wom- en’s Hospital and the Monash Medical Centre, Melbourne. Exclusion criteria included age less than 18 or more than 70 years, inability to speak/read English, diagnosis .12 months before, and the pres- ence of known intracranial disease or cognitive impairment. After obtaining written consent, patients engaged in a 15-min interview about demographic and illness information. At the end of the interview, patients were given a questionnaire pack, which they completed at home and returned by mail. After excluding those women who did not complete all ele- ments of the study, the sample was reduced to 100 women. Patients (N ¼ 100) were aged between 20 and 70
- 8. years (mean ¼ 52.52, SD ¼ 12.17), and were within a year ’s diagnosis of GC at interview (mean weeks since diagnosis ¼ 22.21, SD ¼ 14.58). The women were predominantly Australian born (71%), and the major- ity of patients (70%) were married, with 80% having had children. In terms of religion, 42% of the sample was Christian, 33% Roman Catholic, 19% reported having ‘‘no religion,’’ and 6% ‘‘other.’’ Disease charac- teristics are presented in Table 2. Measures Depression was measured using the Beck Depression Inventory for Primary Care(34), anxiety was assessed using the State Anxiety Scale from the Spielberger State Trait Anxiety Inventory(35), and spirituality was assessed using the Spiritual Involvement and Beliefs Scale-Revised(36). The Spiritual Involvement and Be- liefs Scale-Revised comprises 22 items that examine Table 1. Positive and negative spiritual coping methods Positive spiritual coping methods Explanation Negative spiritual coping methods Explanation Benevolent religious reappraisal Redefining the stressor through religion as benevolent and potentially beneficial Spiritual discontent Expressions of confusion and
- 9. dissatisfaction with God Collaborative religious coping Seeking control through a partnership with God in problem solving Interpersonal spiritual discontent Expressions of confusion and dissatisfaction with clergy or members Seeking spiritual support Searching for comfort and reassurance through God’s love and care Punishing God reappraisal Redefining the stressor as a punishment from God for the individual’s sins Religious forgiveness Looking to religion for help in letting go of anger, hurt, and fear associated with an offense Demonic reappraisal Redefining the stressor as the act of the Devil Spiritual purification Searching for spiritual cleansing through
- 10. religious actions Reappraisal of God’s powers Redefining God’s powers to influence the stressful situation Spiritual focus Seeking relief from the stressor through a focus on one’s religion or spirituality Spiritual connection Seeking a sense of connectedness with transcendent forces Adapted from Pargament et al.(30, p711). Table 2. Disease characteristics (N ¼ 100) Characteristic Options for response N Cancer site Endometrium 38 Ovary 32 Cervix 23 Vulva 5 Vagina 1 Fallopian tube 1 FIGO staging I 60 II 11 III 28 IV 1 Treatment type Surgery 87 Chemotherapy 41 Radiotherapy/brachytherapy 25
- 11. None 1 Currently in active treatment Yes 20 No 80 Contribution of spirituality to mood in women with gynecological cancer 757 # 2005 IGCS, International Journal of Gynecological Cancer 15, 755–761 rituals and belief in a higher power, internalized beliefs and spiritual growth, meditation and existential beliefs, and humility and daily application of spiritual princi- ples(36). The Brief RCOPE of Pargament et al.(30) was used to assess positive and negative spiritual coping. The Brief RCOPE comprises 14 items that divide into two subscales, positive and negative religious coping. The creators of the scale advise that the Brief RCOPE is applicable to ‘‘a wide range of Judeo-Christian groups . [and] may be applicable to members of other ethnocentric religions as well, such as Islam’’(30, p722). To make the scale more acceptable to nonbelievers of the main monotheistic religions, certain aspects of the scale were altered; in particular, in addition to the word God, the phrase, a power greater than myself was added. Statistical analyses Data were analyzed using SPSS 10.0.7. Two sequential regression analyses were employed to determine whether spirituality (step 2) and then positive and negative spiritual coping (step 3) accounted for any of the variance in anxiety and depression, over and
- 12. above the variance accounted for by illness and demo- graphic variables (step 1). The illness and demo- graphic variables (ie, age, presence of ovarian cancer relative to other forms of GC, active treatment vs no active treatment, stage of disease—I or II vs III or IV, and having had chemotherapy) were selected a priori, according to the findings of past research. After data screening, one multivariate outlier was removed (reducing the data set to N ¼ 99), and skewed varia- bles were transformed to meet assumptions. Results Use of the published cutoff scores of the Beck Depres- sion Inventory for Primary Care(34) revealed that 24% of the sample exhibited at least mild symptoms of depression (13% of the sample had mild symptoms, 6% moderate symptoms, and 5% severe symptoms). The mean anxiety score was 38.56 (where a higher score indicates a greater level of anxiety), compared with a mean anxiety score for women in the general population (aged between 40 and 69) of 34.35(35). The correlation coefficients among illness variables were in the expected direction (eg, presence of ovarian cancer correlated with having had chemotherapy) and ranged from .50 to .70. In the first regression (Table 3), depression scores served as the criterion variable. R was not significantly different from zero at the end of steps 1 or 2 but was significantly different from zero after step 3. Step 1: R ¼ .31, F(5,93) ¼ 1.92, P ¼ .098; step 2: R ¼ .31, F(6,92) ¼ 1.61, P ¼ .153; and step 3: R ¼ .53, F(8,98) ¼ 4.37, P , .01. In the final model, the predictors ac- counted for 28% of the variance in depression scores,
- 13. change statistics: R2 ¼ .28, F(2,90) ¼ 11.54, P , .01. Specifically, younger age, later stage of disease, and greater use of negative religious coping predicted significantly a higher level of depression. Although not statistically significant, spirituality made a strong contribution to the variance in depression scores (b ¼ 2.378, P ¼ .053), whereby a lower level of spiritu- ality was associated with a higher level of depression. In the second regression (Table 4), anxiety served as the dependent variable. Predictors were entered as for the first regression. After each of the three steps, R was not significantly different from zero (P . .10). Nonetheless, we examined the change statistics and unique contributions from each of the predictors. We found that the addition of positive and negative spiri- tual coping to the equation resulted in a significant improvement in the model, change statistics: R2 ¼ .12, F(2,90) ¼ 4.33, P , .05. Negative spiritual coping was the only significant predictor of anxiety scores Table 3. Summary of final model from the sequential regression analysis for variables predicting transformed depression scoresa Variable B Standard error of B b t P Age 2.017 .008 2.185 22.015 .047* Ovarian cancer .201 .294 .086 0.684 .496 Phase of treatment .086 .337 .032 0.255 .800 Chemotherapy .188 .291 .084 0.644 .521 Stage of disease .632 .276 .264 2.293 .024* Spirituality 2.015 .008 2.378 21.959 .053 Positive spiritual copingb 29.020 4.891 2.365 21.844 .068 Negative spiritual copingb 214.766 4.128 2.352 23.577 .001** aSquare root transformation applied.
- 14. bInverse transformation applied. *P , .05. **P , .01. 758 N. Boscaglia et al. # 2005 IGCS, International Journal of Gynecological Cancer 15, 755–761 (b ¼ 2.25, P , .05), whereby more negative spiritual coping was associated with higher levels of anxiety. Discussion This study was conducted to examine the contribution of spirituality and positive and negative spiritual cop- ing to mood in women within a year ’s diagnosis of GC. Our results indicate that almost one quarter of the sample experienced at least mild depressive symp- toms and that levels of anxiety were higher than that of women in the general population. Our findings also show that among women diagnosed with GC within the past year, those who were younger, had more advanced disease, and who used more negative spiri- tual coping had a greater tendency towards depressed mood, and, although not statistically significant, patients with lower levels of spirituality also tended to be more depressed. The use of negative spiritual cop- ing was associated with greater anxiety scores. Turning first to the predictive role of age in mood outcomes in GC, our results are not surprising. Youn- ger women treated for GC may face the added stress of potential infertility or be concerned about the future
- 15. of their families/children, thus, placing younger women at increased risk for psychological distress(7). Indeed, research has demonstrated that among women with ovarian cancer, younger patients (,50 years) were more likely to be depressed than older patients(6). Later stage of disease was another significant pre- dictor of depression in our sample; this is in agreement with research findings that indicate that among women with GC (and cancer patients in general) more advanced disease is associated with higher levels of depression(4,9). On the other hand, we found that phase of treatment (active treatment vs no current treatment) and site of GC (ovarian vs nonovarian GC) were not predictive of depression or anxiety. These findings contrast with the findings of other studies(4–6,8) and may be reflective of the high degree of support provided to women in the active phase of treatment. Indeed, many studies have found that social support is protective against mood disturbance(37). In this study, the use of negative spiritual coping significantly predicted depression and anxiety, and there was a near significant (P ¼ .053) trend for lower levels of spirituality to be predictive of higher levels of depression. This is consistent with extant research in which an association between higher levels of spirituality and good psychological adjustment to cancer(17–20) has been demonstrated. Findings such as these are typically explained by the hypothesized ‘‘stress buffering’’ and ‘‘meaning-making’’ role of spiri- tuality. Kim and Seidlitz(38) suggest that spirituality can buffer the effects of stress through its influence on thinking, emotions, and behavior. They argue that
- 16. spiritual beliefs may help a person to find meaning in life, thus limiting the mental health consequences of adverse experiences. God and related religious and philosophical systems may offer a type of schemata for explaining and predicting the vacillating course of cancer(39), thus helping to give the illness meaning and perspective and to provide answers to existential questions that arise(40). Spiritual practices can also fos- ter the development of supportive social networks and thus promote health behaviors and reduce nega- tive emotions(38). In addition, spiritual beliefs, in the sense of beliefs related to a connection to something bigger than the self, can help cancer patients tolerate the difficulties of their illness(41). It appears then that for women who are spiritually inclined, spirituality may function as an important resource during the course of GC. What, then, of the finding that negative spiritual coping significantly predicted both depression and anxiety in our sample? As stated, the use of negative spiritual coping expresses a less secure relationship Table 4. Summary of final model from the sequential regression analysis for variables predicting transformed anxiety scoresa Variable B SE B b t P Age 2.009 .009 2.094 20.930 .355 Ovarian cancer .061 .332 .025 0.183 .855 Phase of treatment .074 .381 .027 0.194 .847 Chemotherapy .287 .329 .127 0.873 .385 Stage of disease .192 .312 .078 0.616 .540 Spirituality 2.011 .009 2.264 21.234 .221 Positive spiritual copingb 25.776 5.529 2.229 21.045 .299 Negative spiritual copingb 210.505 4.667 2.245 22.251 .027*
- 17. aSquare root transformation applied. bInverse transformation applied. *P , .05. Contribution of spirituality to mood in women with gynecological cancer 759 # 2005 IGCS, International Journal of Gynecological Cancer 15, 755–761 with a higher power and a tenuous and ominous view of the world. Perhaps then, those who use negative spiritual coping methods are mobilizing their spiritual resources ineffectively, translating their spiritual be- liefs into unhelpful strategies that promote (rather than protect from) depression and anxiety. However, given that the study was cross-sectional, the possibil- ity that the participants’ psychological distress pre- ceded the use of negative religious coping methods cannot be excluded. In addition to its cross-sectional design, another lim- itation to the present study is the lack of consideration of other variables that may predict mood. In particu- lar, we have not examined the role of non-spiritual coping methods, disposition, or social support in mood outcomes. A larger study that examines the con- tribution of such variables to emotional outcomes and well-being in women with GC is required. Alternately, a qualitative approach, in which women are asked to elaborate on their own methods of spiritual coping, may help elucidate the most important aspects of spir- ituality (if any) for women with GC.
- 18. This study adds empirical evidence to the sugges- tion of Ramondetta and Sills(1) that spirituality is an important consideration in the care of women with GC, and also, raises questions for those working with GC patients: What do I do if my patient is depressed or spiritually distressed? To whom do I refer such a patient? Considering the implications of depression and anxiety, and the contribution of spirituality and spiritual coping to mood outcomes, healthcare pro- viders may need to consider such questions. Acknowledgments We are indebted to Ms Helen Sells for her help with recruitment of participants. References 1 Ramondetta LM, Sills D. Spirituality in gynecological oncology: a review. Int J Gynecol Cancer 2004;14:183–201. 2 Corney RH, Everett H, Howells A, Crowther ME. Psy- chosocial adjustment following major gynaecological surgery for carcinoma of the cervix and vulva. J Psycho- som Res 1992;36:561–8. 3 Thompson DS, Shear MK. Psychiatric disorders and gynecological oncology: a review of the literature. Gen Hosp Psychiatry 1998;20:241–7. 4 Cain EN, Kohorn EI, Quinlan DM, Schwartz PE, Latimer K, Rogers L. Psychosocial reactions to the diag- nosis of gynecologic cancer. Obstet Gynecol 1983;62:635–41. 5 McCartney CF, Larson DB, Wada CY, Cahill P. Effect of
- 19. psychiatric liaison on consultation rates and reasons for consult in gynecologic oncology. J Psychosom Obstet Gynaecol 1986;5:253–61. 6 Bodurka-Bevers D, Basen-Engquist K, Carmack CL et al. Depression, anxiety, and quality of life in patients with epithelial ovarian cancer. Gynecol Oncol 2000;78:302–8. 7 Auchincloss SS, McCartney CF. Gynecologic cancer. In: Holland JC, ed. Psycho-oncology. New York: Oxford Uni- versity Press, 1998:359–70. 8 Klee M, Thranov I, Machin D. Life after radiotherapy: the psychological and social effects experienced by women treated for advanced stages of cervical cancer. Gynecol Oncol 2000;76:5–13. 9 Massie MJ, Holland JC. Depression and the cancer patient. J Clin Psychiatry 1990;51:12–7. 10 Lipowski ZJ. Physical illness and psychopathology. Int J Psychiatry Med 1974;5:483–97. 11 Fava GA, Sonino N. Depression associated with medical illness. CNS Drugs 1996;5:175–89. 12 Graydon JE. Factors that predict patients’ functioning following treatment for cancer. Int J Nurs Stud 1988;25: 117–24. 13 Emblen JD. Religion and spirituality defined according to current usage in nursing literature. J Prof Nurs 1992; 8:41–7. 14 Jenkins R, Pargament K. Religion and spirituality as
- 20. resources for coping with cancer. J Psychosoc Oncol 1995; 13:51–74. 15 Reed PG. An emerging paradigm for the investiga- tion of spirituality in nursing. Res Nurs Health 1992;15: 349–57. 16 Reed PG. Spirituality and well-being in terminally ill hospitalized adults. Res Nurs Health 1987;10:335–44. 17 Schnoll RA, Harlow LL, Brower L. Spirituality, demo- graphic and disease factors, and adjustment to cancer. Cancer Pract 2000;8:298–304. 18 Gioiella ME, Berkman B, Robinson M. Spirituality and quality of life in gynecologic oncology patients. Cancer Pract 1998;6:333–8. 19 Chibnall JT, Videen SD, Duckro PN, Miller DK. Psycho- social-spiritual correlates of death distress in patients with life-threatening medical conditions. Palliat Med 2002;16:331–8. 20 Kaczorowski JM. Spiritual well-being and anxiety in adults diagnosed with cancer. Hosp J 1989;5:105–16. 21 Pargament KI. God help me: toward a theoretical framework of coping for the psychology of religion. Res Soc Sci Study Relig 1990;2:195–224. 22 Pargament KI. The psychology of religion and coping: the- ory, research, practice. New York: Guilford Press, 1997. 23 Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer, 1984.
- 21. 24 Skinner EA, Edge K, Altman J, Sherwood H. Searching for the structure of coping: a review and critique of cat- egory systems for classifying ways of coping. Psychol Bull 2003;129:216–69. 25 Carver CS, Pozo C, Harris SD et al. How coping medi- ates the effect of optimism on distress: a study of women with early stage breast cancer. J Pers Soc Psychol 1993;65:375–90. 26 Schnoll RA, Knowles JC, Harlow L. Correlates of adjustment among cancer survivors. J Psychosoc Oncol 2002;20:37–59. 760 N. Boscaglia et al. # 2005 IGCS, International Journal of Gynecological Cancer 15, 755–761 27 Wagner MK, Armstrong D, Laughlin JE. Cognitive de- terminants of quality of life after onset of cancer. Psychol Rep 1995;77:147–54. 28 Pargament KI, Ensing DS, Falgout K et al. God help me: (I): religious coping efforts as predictors of the outcomes to significant negative life events. Am J Community Psy- chol 1990;18:793–824. 29 Pargament KI, Olsen H, Reilly B, Falgout K, Ensing DS, Van Haitsma K. God help me (II): the relationship of religious orientations to religious coping with negative life events. J Sci Study Relig 1992;31:504–13. 30 Pargament KI, Smith BW, Koenig HG, Perez L. Patterns
- 22. of positive and negative religious coping with major life stressors. J Sci Study Relig 1998;37:710–24. 31 Pargament KI, Ishler K, Dubnow EF et al. Methods of religious coping with the Gulf War: cross-sectional and longitudinal analyses. J Sci Study Relig 1994;33:347–61. 32 Koenig HG. Spirituality in patient care. Philadelphia, PA: Templeton Foundation Press, 2002. 33 Bosworth HB, Kwang-Soo P, McQuoid DR, Hays JC, Steffens DC. The impact of religious practice and reli- gious coping on geriatric depression. Int J Geriatr Psychi- atry 2003;18:905–14. 34 Beck AT, Guth D, Steer RA, Ball R. Screening for major depression disorders in medical inpatients with the Beck Depression Inventory for Primary Care. Behav Res Ther 1997;35:785–91. 35 Spielberger CD. Manual for the State-Trait Anxiety Inven- tory (Form Y). Palo Alto, CA: Consulting Psychologists Press, 1983. 36 Hatch RL, Burg MA, Naberhaus DS, Hellmich LK. The Spiritual Involvement and Beliefs Scale: development and testing of a new instrument. J Fam Pract 1998;46:476–86. 37 Lepore SJ. Social-environmental influences on the chronic stress process. In: Gottlieb BH, ed. Coping with chronic stress. New York: Plenum Press, 1997:133–60. 38 Kim Y, Seidlitz L. Spirituality moderates the effect of stress on emotional and physical adjustment. Pers In- divid Dif 2002;32:1377–90.
- 23. 39 Jenkins RA, Pargament KI. Cognitive appraisal in can- cer patients. Soc Sci Med 1988;26:625–33. 40 Holland JC, Passik S, Kash KM et al. The role of reli- gious and spiritual beliefs in coping with malignant melanoma. Psycho-oncology 1999;8:14–26. 41 Musick MA, Koenig HG, Larson DB, Matthews D. Reli- gion and spiritual beliefs. In: Holland JC, ed. Psycho- oncology. New York: Oxford University Press, 1998: 780–89. Accepted for publication October 14, 2004 Contribution of spirituality to mood in women with gynecological cancer 761 # 2005 IGCS, International Journal of Gynecological Cancer 15, 755–761 Relationship of Religious Beliefs with Anxiety and Depression Aljohara University
- 24. Running head: RELIGION AND MENTAL HEALTH 1 Relationship of Religious Beliefs with Anxiety and Depression BOSCAGLIA, N., CLARKE, D. M., JOBLING, T. W., & QUINN, M. A. (2005). The contribution of spirituality and spiritual coping to anxiety and depression in women with a recent diagnosis of gynecological cancer. International Journal of Gynecological Cancer, 15(5), 755-761. The objective of this study was to work out whether or not, once accounting for religious involvement and beliefs, and positive and negative religious header may account for any of the variations in anxiety and depression among ladies among one year's diagnosing of medical specialty cancer. The author concludes that spirituality and spiritual coping are important to women with cancer and that health professionals in the area should consider these issues. Koenig, H. G. (2009). Research on Religion, Spirituality, and Mental Health: A Review. The Canadian Journal of Psychiatry, 54(5), 283–291. This article talk about the religious and religious factors are more and more being examined in medical specialty analysis. Non secular beliefs and practices have long been joined to hysteria, neurosis, and psychotic delusions. However, recent studies have known another facet of faith that will function a psychological and social resource for dealing with stress. When process the terms faith and spirituality, this paper reviews analysis on the relation between faith and (or) spirituality, and
- 25. psychological state, that specialize in depression, suicide, anxiety, psychosis, and misuse. The results of Associate in nursing earlier systematic review are mentioned, and newer studies within us, Canada, Europe, and alternative countries are delineated. Whereas non secular beliefs and practices will represent powerful sources of comfort, hope, and which means, they're typically elaborately entangled with neurotic and psychotic disorders, typically creating it tough to work out whether or not they are a resource or a liability. Moreira-Almeida, A., Lotufo Neto, F., & Koenig, H. G. (2006). Religiousness and mental health: a review. Revista brasileira de psiquiatria, 28(3), 242-250. This paper reviews the scientific proof offered for the connection between faith and mental state. Conjointly the authors gift the most studies and conclusions of a bigger systematic review of 850 studies on the religion-mental health relationship printed throughout the twentieth Century known through many databases. This paper conjointly includes associate update on the papers printed since 2000, together with researches performed in Brazil and a short historical and method background. And Theoretical pathways of the religiousness-mental health association and clinical implications of those findings are mentioned. Ross, C. E. (1990). Religion and psychological distress. Journal for the Scientific Study of Religion, 236-245. The author did this paper by employing a sample of Illinois residents (and dominant for sociodemographics and disposition to specific feelings). And he found that the stronger an individual's faith, the lower the extent of psychological distress. This supports the concept that faith reduces demoralization and provides hope and that means. However, the author found that persons with no faith likewise had low levels of distress. Thus, there was a curving impact of nonsecular belief on distress. Additionally, the author found that Protestants had very cheap distress levels, followed by Catholics, Jews, and others. Variations in belief systems, however, particularly a belief
- 26. within the Yankee Protestant ethic, didn't make a case for variations in distress among nonsecular teams. The strength of nonsecular beliefs seems to be a lot of vital than content in explaining the impact of faith on psychological distress. Williams, D. R., Larson, D. B., Buckler, R. E., Heckmann, R. C., & Pyle, C. M. (1991). Religion and psychological distress in a community sample. Social Science & Medicine, 32(11), 1257- 1262. This paper examines the result of nonsecular group action and affiliation on psychological distress in a very longitudinal community study of 720 adults. nonsecular affiliation is unrelated to mental state standing. In distinction, though nonsecular group action doesn't directly scale back psychological distress, it buffers the hurtful effects of stress on mental state. That is, within the face of nerve-racking events and physical health issues, nonsecular group action reduces the adverse consequences of those stressors on psychological well- being. Running head:sentencing programs and aggressive tendencies 1 Running head:sentencing programs and aggressive tendencies 2The effect of sentences programs on aggressive tendencies amongst adolescent offenders Student Name Effat University Abstract Purpose: The purpose of this research proposal is to plan and carry out a study that will evaluate the relationship between family attachment and social interaction. Social interaction is of special importance due to how current students spend their time, either between real life social interactions or social
- 27. media.Methods: A cross-sectional design will be employed to measure students’ beliefs, behaviors, and personality at one point in time. Various measures will be given to measure social interaction, family attachments, and personality. Implications: The implications of this study, if it is carried out, is a better understanding of social isolation during a student’s move to a university dormitory. Moreover, if family attachment is found to be associated with better adjustment, then perhaps better inventions can be made to prevent or reduce adjustment problems. Keywords: SocialInteraction, Family Relationships, Adjustment, Moving The effect of sentences programs on aggressive tendencies amongst adolescent offenders Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth. Variable 1 (Dependent Variable) Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth. Variable 2 (Independent Variable) Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and
- 28. you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth. Conceptual Framework Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth. Gaps in Existing Knowledge Base Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth. Purpose of Research Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.
- 29. Research Questions Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Conceptual Definitions Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth. Hypotheses Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth.Start writing something really profound and incredible here. If you do so, perhaps, just perhaps, we might give you an A and you’ll graduate and become the most incredible psychologist to have existed on planet Earth. Proposed MethodsSample Because the best time to establish a habit is considered to be with individual in early adulthood, our target population will be young adults in college. Measures Executive Functioning.Measured by the NIH ToolBox. Measures of working memory, flexible switching, processing
- 30. speed, inhibition, and initiation will be measured to determine the overall level of executive functioning for each subject. Final Numerical Grade. measured by each subject’s cumulative assignments and tests.Design & Procedure A correlational cross-sectional design will be used in order to gather the data and analyze it. Analytic Plan A standard independent samples t-test will be performed to determine statistical significant mean differences on the dependent variables. Anticipated Results We hypothesize that students who receive the intervention of HIT will have higher post-test EF as well as higher final numerical grades. Implications of Results The results from this study will have both practical and theoretical implications. From a practical standpoint, the results will demonstrate that a more practical type of exercise can both be beneficial physiologically as well as academically. Therefore, this approach can accommodate to younger adults who tend to be busy with school and work. From a theoretical perspective, the data can provide very important empirical support for psychological and academic benefits of HIT. References Last Name, F. M. (Year). Article Title. Journal Title, Pages From - To. Last Name, F. M. (Year). Book Title. City Name: Publisher Name.
- 31. Sot Scr Med Vol 3.2, No 11, pp 1257-1262, 1991 Pnnted m Great Bntam All nghts reserved 0277-9536/91 $3 00 + 0 00 Copyright 0 1991 Pergamon Press plc RELIGION AND PSYCHOLOGICAL DISTRESS IN A COMMUNITY SAMPLE DAVID R WILLIAMS,’ DAVID B LARSON,* ROBERT E BUCKLER,.’ RICHARD C HECKMANN~ and CAROLINE M PYLE’ I Departments of Sociology and Epldemlology and Pubhc Health, Yale Umverslty, P 0 Box 1965, Yale Statlon, New Haven, CTO6520, US A, *NatIonal Institute of Mental Health, 5600 Fishers Lane, Rockvdle, MD 20857, U S A, ‘Department of Psychology, Western Seminary, 5511 E Hawthorne, Portland, OR 97215, U S A 4Department of Psycluatry, Umverslty of Colorado School of MedIcme, 4200 E 9th Ave. Denver, CO 80262, U S A and SDepartment of Epldemlology and Pubhc Health, Yale School of Medlcme, 60 College Street, New Haven, CT 06520, U S A Abstract-This paper exammes the effect of [email protected] attendance and affibatlon on psychologlcal distress m a lonptudmal commumty study of 720 adults Rebglous atlibatlon IS unrelated to mental health status In contrast, although rehgous attendance does not directly reduce psychologlcal distress, It buffers the deletenous effects of stress on mental health That IS, m the face of stressful events and physlcal health problems, rebgous attendance reduces the adverse consequences of these stressors on psychologlcal
- 32. well-bemg Key words-rehglon, psychologlcal &stress, stress The relationshIp between rehglon and health status has been recelvmg mcreasmg sclentlfic attention in recent years One mdlcator of this interest 1s the growing number of reviews focused on rehglous vanables that have appeared m the medical and social science hterature [l-7] In terms of mental health outcomes, the literature indicates that more often than not, religion measures are inversely associated with indicators of psychological distress Bergm [S] revlewed 26 studies that assessed the assoclatlon be- tween rehglon and mental health status He reported that almost half of the studies found an inverse assoclatlon between rehglon and psychological symp- toms with the remainder about equally divided be- tween those that found a positive relationship and those that reported no assoclatlon However, given that 80% of the studres reviewed by Bergm [S] utlhzed student samples, it IS difficult to draw conclustons about the generahzablhty of these findings Studies employmg more representative samples present a slmllar mixed pattern of findings Two studies based on national probability samples have reported an inverse assoclatlon between rehglous attendance and psychological distress [8,9] Slml- larly, several community studies have reported m- verse assoclatlons between measures of religion and scores on screening scales of global distress [IO-131 At the same time, other community studies report no assoclatlon between rehglon and mental health status [14-161
- 33. The hterature assessing the mental health conse- quences of rehglon IS plagued with conceptual and methodological hmltatlons which require that great caution should be exercised m mterpretmg the find- mgs For example, with few exceptions [16, 171 most of the existing studies have used cross-sectional designs m which rehglous mvolvement and mental health status are measured simultaneously A given level of psychological functlonmg can be either a cause or a consequence of rehglous behefs and behavior In cross-sectional analyses it 1s lmposslble to detect causal dlrectlonahty m the relatlonshlps observed Researchers have also given inadequate attention to the measurement of the rehglous vanabie and to the underlying processes by which rehglon may affect health status [2, IO, 17-201 One way m which rehglous mvolvement may affect health status 1s by modlfymg the relatlonshlp between stress and illness Stress has been shown to have pervasive negative effects on physical and mental health [21], but psychosocial resources can compen- sate for or moderate the impact of stress on health [22] Recently, Krause and Van Tran [23] docu- mented that rehglous mvolvement 1s a cntlcal psycho- social factor that counteracts the adverse effects of stress on feelings of self-esteem and mastery The literature on stress recognizes that a given psychoso- cial resource, such as rehglon, may affect psychologl- cal distress by directly enhancing mental health status, lrrespectlve of the level of stress, and/or by buffenng the effects of stress on health [22] The buffenng hypothesis postulates that m the face of stress, religion can protect the mdlvldual from the potentially negative consequences of stress To our
- 34. knowledge, there have been no attempts to empln- tally assess the dynamics of the assoclatlon between religion, stress and psychological distress This paper seeks to enhance our understandmg of the relatlonshlp between rehglous behavior and mental health by exammmg how two measures of rehglous mvolvement, rehglous attendance and reh- glous affiliation, combme with stress to affect psycho- logical distress In 1967, a random sample of rest- dents of metropolitan New Haven were mtervlewed Lmdenthal et al [13] have reported on the cross- sectional assoclatlons between rehglon and mental health status They found that both rehglous affiha- tlon and rehglous attendance were inversely assocl- 1257 1258 DAVID R WILLIAMS et ~1 ated with psychological distress Two years later, a second wave of data was collected from these New Haven residents To date, no analyses have related the 1967 religion measures to distress m 1969 In addition, although controls were utilized for SOCIO- demographic vanables m the ongmal study, no attempts were made to assess the extent to which the assoclatlon between religion and psychological distress vanes for structural charactenstlcs such as race or socloeconomlc status A growing body of evidence indicates that stress, the resources to cope with stress, and the efficacy of these resources vary for groups occupying different structural positions m society [22]
- 35. This paper focuses on the ongmal respondents who were reinterviewed m 1969 We assess the extent to which the pattern of findings m the cross-sectional analyses remam robust m the more ngorous prospec- tive analyses Specifically, we address the followmg research questions 1 How do religious attendance and affiliation relate to psychological distress? 2 Do the consequences of religious mvolvement vary by major soclodemographlc charactenstlcs such as age, race, education and gender7 3 To what extent can measures of rehglous mvolvement buffer or moderate the effects of stress on health? METHODS The analyses reported here use data from the Myers et al [24,25] lonBtudma1 study of mental health m New Haven, Connecticut The sample con- sists of 720 adults who were reinterviewed m 1969 from an ongmal random sample of 938 respondents who were first interviewed m 1967 Table 1 lists the means, standard deviations and mtercorrelatlons among the vanables utilized Our sample IS 44% male, 11% black, 26% unmarned, and has a median education level of 12 years and a mean age of 44 8 years Psychological distress 1s measured by the Gurm ef al [8] symptom checklist scale This scale consists of 20 statements of psychophysiological symptoms
- 36. that indicate the presence of moods of depression and anxiety. The symptoms of the Gurm scale were selected from among those most frequently mentioned by patients m treatment and they allow for respondents to be ordered on a contmuum of reported distress Respondents reported the fre- quency with which each symptom was expenenced Scores on the Gunn scale thus range from 20 (all symptoms expenenced ‘often’) to 80 (all symp- toms occurrmg ‘never’) In contrast to our use of the Gunn scale as a contmuous measure, the scale 1s sometimes used qualitatively to dlstmgmsh between the mentally impaired (score = 66 or lower), and the non-impaired We believe that our contmuous measure of psycholoDca1 distress 1s more theoreti- cally appropnate for the study of the assoclatlon between religion and mental health than a more qualitative dlstmctlon between psychlatnc cases and normals If rehglon has positive effects on mental health, they are hkely to be evident throughout the continuum of mental health status and not only at the extreme of the dlstnbutlon Two measures of rehglous commitment at wave one (1967) are utilized Religious attendance measures the usual frequency of attending rehglous services (values range from 1 = never to 6 = more than once a week) To facilitate interpretation of product terms m the regression analyses, the religious attendance measure was converted to a standard score based on the mean and standard devlatlon of the total sample, and a constant was added to this standardized vanable so that the lowest actual value 1s zero The religious affiliation measure IS based on the response to the questlon “Are you
- 37. affiliated with any church or religious group?” (1 = yes, 0 otherwise) Two summary measures of stressful life expen- ences, occurnng dunng the two years between the mtervlews, are utlhzed Both measures of stress are listed m the Appendix The first 1s an index of undesirable life events The second stress measure 1s a sum of the number of physical health problems experienced To avoid confounding between the measure of psychological distress and the health problems index, followmg Kessler and Cleary [26], we excluded those health complamts that mtultlvely appeared to have a strong psychosomatic compo- nent From a list of 44 symptoms, we selected those 16 health complamts for which a psychosomatic component would be muumal Ordinary least squares (OLS) regression analyses utlhzmg the regression program m SAS [27] are used for estimating the magmtude and statistIca slgmficance of the relatlonshlps among religious Table I Means, standard dewatmn and mtercorrelatmns (dwmals onutted) among vdrldbles I 2 3 4 5 6 7 8 9 IO II I2 Standard Mean dewauon I Age - 2 Education’ -39 - 3 Marital staus (married) -08 06 - 4 Gender (male) IS 05 I4 5 Race (black) -15 -15 -20
- 38. 6 Attendance 1961 -01 09 03 7 Attendance 1969 03 02 02 8 Health problems 20 -15 -07 9 Life events -II -04 -01 10 Gunn 1967 06 I5 I2 II Gunn 1969 00 I5 06 I2 Affihauon 1967 02 I2 08 - -09 -10 -13 02 -01 I4 IO -04 44 81 I6 61 3 37 I 50 074 044 044 0 50 - 0 II 0 32 -01 - I68 100 -01 54 - 219 100 08 -06 -08 - 0 73 0 97 07 -04 -06 14 - 0 82 I I4 -12 17 I4 -27 -15 - 72 05 8 I9 -03 IO I2 -37 -32 53 - 72 85 7 74
- 39. 00 41 27 -04 -01 09 02 - 0 75 049 ‘The education vanable IS coded as follows 1 = less than 7 years, 2 = 7-9 years, 3 = 10-11 years, 4 = 12 years, 5 = 13-15 years, 6 = college graduate and 7 = graduate on professional tranung Rehgon and psychologrcal dtstress m a commumty sample 1259 mvolvement, stress and psychological distress OLS regression is fully appropnate for our continuous dependent vanable The correlation matnx from whtch the regression models were estimated is pre- sented m Table 1 Pauwtse present correlations were used m all regression analyses The analyses pro- ceeded m a senes of steps m which we estimated the effects of rehgrous mvolvement on psychological distress This relationship was then adlusted for potentially confounding sociodemograpmc factors The soctodemographrc vanables utrhzed are age (m years), education (nommally scaled vanable coded from 1 = less than 7 years of education to 7 = graduate or professtonal training), gender (1 = male), manta1 status (1 = marned, 0 otherwtse), and race (1 = black, 0 otherwtse) Subsequent regression models assessed the association between stress and psychological distress and the extent to which rehgtous mvolvement may buffer the effects of stress on health A final step m all analyses mvolved entenng the Time 1 Gunn score as a predictor of Time 2 Gunn The use of the Ttme 1 distress measure effectively
- 40. converts the Time 2 outcome mto change scores, Thts 1s appropnate m these analyses because tt allows us to determine the extent to whtch any improved mental health functiontng found among those high on rehgtous mvolvement ts stgmficantly greater than any improvement found among those having lower scores on the rehgion measures RESULTS Relrglon and psychologrcaI dzstress Table 2 presents the results of three regression analyses that assess the assoctation between psycho- logical distress and religion In the first model, Ttme 2 (1969) Gunn scores are regressed on the Time 1 (1967) religious attendance and affihatton In the second regression model, controls are introduced for soctodemographtc factors (age, education, manta1 status, gender and race) that were measured at Time 1 The final model adds the Time 1 (1967) Gunn score as a predictor of the Time 2 Gunn score The first model m Table 2 indicates that although rehgtous affiliation IS unrelated to psychological drs- tress, rehgrous attendance IS positively associated with the Time 2 (1969) Gunn score Persons who attend rehgtous services regularly report lower levels of psychologtcal distress than infrequent attenders and non-attenders This relattonshtp remains robust when adlusted for the soctodemographtc variables but tt IS reduced to non-stgmficance when controlled for Time 1 (1967) psychologtcal distress Religious attendance at Time 1 is not associated with increases m psychologtcal well-being, as measured by the Gurm scales. Thus, m the face of ngorous statistical con-
- 41. trols for the possible confounding of public rehgtous partictpatton with scores on the Gurm scale, we find that attendance IS unrelated to psychological d:stress Our prospecttve analyses have failed to replicate the inverse assoctattons between religious commitment and psychologtcal distress that were reported for the cross-secttonal analyses at Time 1 [ 131 We tested for nonhneanty m the assoctatton be- tween rehgtous attendance and mental health status Table 2 Analyses of the assoclatlon between Tune 2 (1969) Gunn scores and the rehgton measures at Tlmc 1 (1967) i II III Independent vanables (SE) (A) (& Attendance 0 83’. 0 84.’ 0 16 (0 32) (0 32) (0 28) Affihatlon -046 -0 88 -0 88 (0 75) (0 74) (0 64) Age 003 (0 02) (%5 Education 0 94.1 0 48’. (0 22) (0 19) Mamed 0 87 0 II (0 69) (0 60)
- 42. Sex (men= 1) I 60** 0 54 (0 60) (0 52) Race (black = 1) 0 63 I 30 (0 97) (0 84) Gunn 1967 0 49” (0 03) Constant 71 80 66 14 35 81 R2 0010 0 050 0290 ** = P < 0 01, 2-taded tests b = unstandardized regrewon coefficients Shaver et al [28] reported a curvihnear relatton- ship between religion measures and psychologtcal symptoms The very rehgtous and the non-rehgtous enloyed the best reported health Accordingly, to a regression equation that included the demographic vanables and Ttme 1 (1967) rehgious attendance, we added the squared coefficient for religious attend- ance (quadratic term) A srgmficant quadratic term would indicate that the associatton between rehgtous attendance and distress ts curvtltnear The quadrattc term was not stgmficant (analysts not shown), mdicat- mg the absence of curvihneanty m the assoctatton between religion and psychological distress We also explored the extent to which vanattons exist by race, gender and educattonal level m the assoctatton between the rehgton measures and psychological distress Specifically, for each of these soctodemographtc vanables, we regressed Time 2 (1969) Gunn scores on the two religion vanables, all
- 43. of the soclodemographlc vanables, and the relevant muthphcatlve term for the interaction between each rehgion measure and the soclodemographlc correlate under consideration In these analyses (not shown), none of the interaction tests were slgmficant In cross-sectional studies researchers frequently assume that the reported level of rehglous mvolve- ment IS a stable characteristic of the respondent In contrast, religious behavior may be a fairly transient phenomenon Lmdenthal et al [ 131, for example, noted that when faced with stress, respondents reported a decline m rehgtous attendance The fact that we are workmg with panel data allows us to explore the nature of changes m rehgtous attendance between 1967 and 1969 and the consequences that these changes could have for mental health status Ftrst, we noted that attendance levels were relattvely stable over the course of 2 years Table 1 reveals that the correlation between rehgtous attendance at Time 1 (1967) and Time 2 (1969) was 0 54 Second, we divided our sample mto subgroups based on the combmatlon of the level of rehglous attendance reported at Ttme 1 (1967) and Time 2 1260 DAVID R WILLIAMS et al (1969) At each tzme point, all respondents were classified into one of three categories. high attenders (persons who attended rehgzous services once a week or more), moderate attenders (zndzvzduals who attended once a month to two or three times a month) and low attenders (those who never attended as
- 44. well as those who attended a few times a year or less) Respondents were then assigned to one of five categones based on their 1967 and 1969 attend- ance. The stub/y hzgh group (n = 216) consists of persons who were hzgh attenders at both time points The newly hzgh (n = 70) are hzgh attenders m 1969 who were either moderate or low attenders m 1967 The declznzng attendance group (n = 99) 1s com- pnsed of hzgh attenders at Tzme I who were moderate or low attenders at Time 2 The moderate group (n = 152) consists of persons who were moderate attenders at both time pomts, as well as those who fluctuated from the moderate to low level or vice versa between the two data collectzon points Finally, the stably low (n = 149) were low attenders at both time points Table 3 presents the results of analyses that exam- med the relatzonshzp between attendance patterns and psychologzcal distress. We anticipated that those who reported conszstently high levels of attendance and those who increased then attendance would have lower levels of [email protected] distress than persons with consistently low attendance levels The first model m Table 3 indicates that the stably high, the newly hzgh and the declzmng attendance group all had szgmficantly higher scores on the Gurm scale (that zs, less psychologzcal distress) than the stably low attendance group Thus, a high level of rehgzous attendance m 1967 or m 1969, irrespective of their attendance level at the other tzme point, zs predictive of psychologzcal well-being However, szmzlar to the findings m Table 2, these assoczatzons do not remam szgnzficant when adJusted for Tzme 1 (1967) distress scores
- 45. Relzgzon, stress and mental health We have noted that rehgzon does not directly enhance the psychologzcal well-being of zts adherents Table 3 Analyses of the assOclauon between Time 2 (1969) Gunn scores and attendance at Time I (1967) combmed wth Time 2 (1969)’ I II Independent vanables (Si (A) Rehgmus attendance a Stably high 1 63. 0 23 (0 73) (0 67) b Newly high 2 06’ 0 58 (0 99) (0 90) c Dechnmg I 90. 041 (0 88) (0 ‘30) d Moderate 0 68 001 (0 79) (0 71) e Stably low (omnted) Time I Gunn 0 40” (0 03) Constant RZ l P < 0 05. l *P < 0 01, 2-taded tests
- 46. ‘Both models mclude controls for age, education, manta1 status, gender and race b = Unstandardized regressIon coefficients We now turn to examme the buffenng hypothesis Can rehgzon protect mdzvzduals from at least some of the negative consequences of stress’ Table 4 presents four models that explored the assoczatzons among rehgzon, stress and psychologzcal distress The use of the Time 1 measures of religion m these analyses excludes the posszbzhty that any modifying effects that we observe are due to changes m rehgzous mvolvement resulting from stress The first model shows the assoczatzon of the two stress measures and the two rehgzon measures to the Time 2 (1969) Gunn scale, controlhng for the soczodemographzc vanables The second model adds adJustment for the Time 1 (1967) Gunn score, and models three and four tests for mteractzons between relzgzous attendance and hfe events, and attendance and health problems, respectively Table 4 shows that both hfe events and health problems are szgnzficantly inversely associated with scores on the Gunn scale As expected, stress IS posrtzvely related to psychologzcal distress Model II indicates that the coefficients for stress are reduced Table 4 Analyses of the assoclatlon between Time 2 (1969) Gunn scores. Time I (I 967) measures of rehgon and mdlcators of stress’ Independent vanables
- 47. I b (SE) II (Sk 111 b (SE) Attendance Afiihatlon Life events (LE) Health problems (HP) Gurm 1967 0 62’ (0 28) -084 (0 66) - I 77’ (0 23) -2 69’. (0 28) Attendance x LE
- 48. 0 II (0 26) -083 (0 59) -1 53” (0 21) -I 85.. (0 26) 0 39’9 (0 03) -023 (0 30) -087 (0 59) -2 26” (0 40) -1 88. (0 26) 0 39’. (0 03) 0 43’ -0 32 (0 32) -065
- 49. (0 60) -I 55” (0 21) - 2 70” (0 44) 0 40.’ (0 03) (021) Attendance x HP 0 52. (0 23) Constant 70 11 44 53 45 4 453 R’ 0 251 0 399 0 403 0404 l P < 0 05, l *P < 0 01, 2-taded tests ‘All models m&de controls for age, education, manta1 status, gender and race b = unstandardued regresston coefficients Rehgon and psychologxal distress m a commumty sample 1261 but remam slgnrficant when controlled for Time 1 (1967) psychologtcal distress Model II also reveals that the relationship between attendance and distress IS reduced to non-sigmficance when controlled for Tl distress Models three and four reveal that both of the multtphcative terms for interactions between stress and rehgious attendance are significant The interaction terms capture operant religious effects that would go unnoted otherwise Moreover, the
- 50. sign is positive for both mteraction coefficients This pattern of results reflects classic buffenng effects That is, at low levels of religious attendance, stress IS associated with increased levels of psychological distress However, as the level of religious attendance increases, the adverse consequences of stress are reduced Surular analyses for the associatton between religious affiliation and the stress measures were not significant In sum, consistent with other research [7], we find that our measure of rehgious behavior (religious attendance) is more consequential for health status than our mdicator of rehgious affiliation The affiha- tion measure is unrelated to psychological distress In contrast, although rehgious attendance does not directly reduce psychological distress, it does buffer the impact of stressful life events and physical health complamts on psychological well-being DISCUSSION The findings reported here underscore the import- ance of giving more systematic research attention to the consequences of rehgious beliefs and behavior for health and well-being. National surveys reveal the contmumg importance of public and pnvate rehgtous mvolement m contemporary Amencan hfe [29] Our results indicate that rehgion may be a potent coping strategy that facihtates adjustment to the stress of hfe Further exploration of this issue merits serious and sustained research attention One compellmg reason to replicate the analyses reported here is the possibihty that they may reflect period or cohort effects The data utilized m this
- 51. study are over 20 years old It is possible that the findings documented here are true only for that earlier time period and would not apply today In a comprehensive review of the literature on rehgious involvement and sublective well-bemg, Wetter et al. [30] found a stronger relationship between religion and SubJective well-being m earlier studies than m more recent ones Our use of longitudmal survey data is clearly an improvement over merely studying cross-sectional associations but analyses of two wave panel data are not without serious hnntanons [31] For example, the inclusion of Time 1 health status adjusts for baseline differences among respondents m the levels of health However, if health status at Time 2 IS also affected by other unmeasured causes, the Time 1 health status indicator IS an inadequate proxy for the mynad factors that are not mcluded m the prediction equation The presence of measurement error is another serious hmitation Errors of measure- ment can create spurious covanance among the variables in the regression models Theoretically- grounded research that utilizes multiple indicators of religion and that employs structural equation modeling procedures [32] can begm to address these lirmtations This paper also illustrates some of the cnucal shortcommgs m current research on religion and mental health Rehgious attendance and religious affiliation are the only measures of religious commit- ment that we utihzed These are two of the most commonly used measures m research on religion [l] In contrast, religious mvolvement is a complex multi-
- 52. dimensional phenomenon [33-351 Kmg and Hunt [33], for example, have tdentified more than a dozen different ways of being rehgious, and have developed and tested scales to measure each component &ml- larly, Levm and associates [2.6,20,36] have pro- posed numerous theoretically mformed mechamsms by which religion can affect health status that clearly constttute the most fruitful extant starting ground for empirical mvestigations of the effects of religion on health. The advancement of our understandmg of the nature of the association between religion and health, is contingent on efforts to comprehensively assess religion, and identify the cnttcal dimensions of reh- gious commitment that are linked to health status Research efforts of thts kmd are necessary to understand even the results presented here We reported that religious attendance buffers or moder- ates the relationship between stress and health How- ever, we are unable to tell if this effect 1s hnked to anything mtnnsmally rehgtous Although we employ controls for formal education m all of the analyses, it IS still possible that the attendance measure is a proxy for some aspect of social status Sociologists have long noted that religious partici- pation IS frequently a badge of socioeconomic status, secular m character, and of no greater rehgious sigmficance than participation m other community orgamzations [37] And there is abundant evidence that participation m formal and informal social groups, rehgious and non-rehgious, can promote health, reduce stress and buffer the effects of stress on health [22] Moreover, besides social class, rehgious attendance may be confounded with functtonal health [36]
- 53. It follows that a simple measure of the frequency of religious attendance does not adequately cap- ture public religious participation A comprehensive assessment of public rehgious mvolvement must include attendance at rehgious meetings other than the main weekly worship service, financial support of religious organizations, and holdmg leadership and volunteer positions m rehgious groups [35]. Researchers must then seek to identify how these public aspects of rehgious mvolvement relate to pn- vate dimensions of religious beliefs and behavior and how they combme to affect levels of health and well-being. Acknowledgements-An earlier version of this paper was presented at the Ntnety-Seventh Annual Meettngs of the Amertcan Psychologtcal Assoctatton, New Orleans, August, 1989 We wish to thank Jerome K Myers for permIssIon to use the data and the anonymous renewers for very helpful comments on an earlier version of this paper. The research was supported, m part, by grant Rl l-8812285, from the National Science Foundation 1262 DAVID R WILLIAMS er al 1 2 3 4 5
- 55. Larson D , Pattlson M , Blazer D , Omran A and Kaplan B Research on rehgous vanables m four major psychlatnc Journals Am J Psychlat 143, 329-334, 1986 Levm J S and Vanderpool H Y Is frequent rehgous attendance really conducive to better health? toward an epidemiology of rehgon Sot Scr Med 24, 589-600, 1987 Jarvls G K and Northcott H C Rehglon and dlffer- ences m morbidity and mortality Sot- .%I Med 25, 813-824, 1987 Schlller P L and Levm J S Is ther a [email protected] factor m health care utlhzatlon7 a review Sot Scl Med 27, 1369-1379, 1988 Bergm A E Rehgloslty and mental health a crmcal reevaluation and meta-analysis Prof Psycho1 14, 170-184, 1983 Levm J S and Schlller P L Is there a rehgous factor m health? J Rehg Hlth 26, 9-36, 1987 Gartner J , Larson D B , Allen G D and Gartner A F Religious commitment and psychopathology a review of the empmcal literature J Psycho1 Theo1 In press Gunn G , Veroff J and Feld S Amerwans View thezr Mental Health Basic Books, New York, 1960 Veroff J , Douvan E and Kulka R The Inner Amerzcan Basic Books, New York, 1981 Idler E L [email protected] mvolvement and the health of the elderly some hypotheses and an mlhal test Sot Forces 66, 226-238, 1987 Petersen L R and Roy A Rehglowty, anxiety and meaning and purpose rehgon’s consequences for psychologlcal well-bemg Rev Rehg Res 27, 49-63, 1985 Hannay D R Rehglon and health Sot Scl Med 14A,
- 56. 683-685. 1980 Lmdenthal J J , Myers J K , Pepper M and Stern M S Mental statuss and rehglous behavior J Scl Study Rehg 9, 143-149, 1970 Brown D R and Gary L E Stressful hfe events, social support networks, and the physical and mental health of urban black adults J Hum Stress 13, 165-174 Carr L G and Hauser W J Class, [email protected] par- ticlpatlon and psychlatnc symptomology Znt J Sot Psychtat 27, 133-142 Clearly P D and Houts P S The psychological impact of the three mile island mcldent J Hum Stress 10, 28-34, 1984 Markides K S , Levm J S and Ray L A Rehglon, agmg, and life satlsfactlon an eight-year, three-wave lonmtudmal studv The Geront 27. 660-665. 1987 Kaplan B and Blazer D G Rehg&n m the’stress and adaptation paradigm In Soctophyslology of Social Re- lattonshlps (Edited by Barchas P ) In press Martin J E and Carlson C R Spmtual dimensions of health psychology In Behavtor Therapy and Relrgron (EdIted bv Miller W R and Martm J E ). DD 57-l 10 Sage, Palb Alto, CA, 1988 I . . Levm J S Religious factors m aging, adlustment, and health a theoretlcal overview J Rehg Agrng 4, 133-146, 1987 Elliott G R and Elsdorfer C Stress and Human Health Spnnger, New York, 1982 Wllhams D R and House J S Stress, social sup- port, control and copmg a social epldemlologlcal view In An Introduction to Health Promotron Research (EdIted by KIckbusch I and Badura B ) World Health Organization In press
- 57. 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 Krause N and Van Tran T. Stress and rehgous mvolve- ment among older blacks J Geront 44, 54-513, 1987 Myers J K, Lmdenthal J J , Pepper M P and Oitrander D R Life events and men&l status a long- tudmal studv J Hlth Sot Behav 13. 398-406. 1972
- 58. Myers J K, Lmdenthal J J and Pepper M ‘P Life events, social integration and psychlatnc symptomatol- ogy J Hlth Sot Behav 16, 421-427, 1975 Kessler R C and Cleary P D Social class and psycho- logcal distress Am Sot Rev 45, 463478, 1980 SAS Institute SAS User’s Gwde Statrstlcs SAS mstl- tute, Gary, NC, 1985 Shaver P , Lenauer M and Sadd S Religiousness, conversion, and subjective well-being Am J Psychrar 137, 1563-1568, 1980 Gallup Report Relrglon m America-50 Years Pnnce- ton [email protected] Research Center Prmceton, NJ Witter R A, Stock W A, Okun M A and Hanng M J Rehglon and SubJective well-being m adulthood a quantitative synthesis Rev Relrg Res 26, 332-342. 1985 Kessler R C , Greenberg D F Lmear Panel Analysis Models of Quantltatlve Change Academic Press, New York, 1981 Joreskog K G and Sorbom D LISREL Esttmarron of Linear Structural Equation Systems by Maximum Llkebhood Methods International Educational Services, Chicago, 1976 Kmg M B and Hunt R A Measunng the rehgous vanable national replication J Scz Study Rehg 14, 13-22, 1975 Mmdel C H and Vaughn C E A multldlmenslonal approach to reltaosity as disengagement J Geronr 33, 103-108, 1978 Amlay S C and Smith D R Agng and rehgous partlclpatlon J Geronf 39, 357-363, 1984 Levm J S and Vanderpool H Y Is rehglon thera- peutically significant for hypertension? Sot Scl Med 29, 69-78, 1989 Goode E Social class and church participation Am J Sot 72, 102-111, 1966
- 59. APPENDIX Life events Measures of Stress The 28 undesirable events are (1) failed school or trammg program, (2) problems m school, (3) moved to a worse nelghborhood, (4) wldowed, (5) divorced, (6) separated, (7) trouble with m-laws, (8) serious physical illness, (9) serious injury or accident, (10) death of a loved one, (11) stdlblrth, (12) frequent minor illness, (13) mental illness, (14) death of a pet, (15) demoted or changed to a less responsible Job, (16) laid off temporarily, (17) busmess faded, (18) trouble with boss, (19) out of work for over a month, (20) fired, (21) financial status a lot worse than usual, (22) foreclosure of mortgage or loan, (23) appearance m court, (24) deten- tion m Jail, (25) arrested, (26) law suit or legal action, (27) loss of dnver’s license, and (28) change m relations with neighbor, friend and relative such as serious or maJor disagreement Health problems The 16 health problems are (I) eye trouble, (2) ear trouble, (3) sinus trouble, (4) throat trouble, (5) bronchitis, (6) pneumoma, (7) tuberculosis, (8) bolls and abscesses, (9) diabetes, (10) kidney trouble, (11) bodily injury, (12-14) operations, (15) cancer or tumors, and (16) tooth trouble, excluding routme prophylaxis In Review
- 60. Research on Religion, Spirituality, and Mental Health: A Review Harold G Koenig, MD 1 Key Words: religion, spirituality, depression, anxiety, psychosis, substance abuse Despite spectacular advances in technology and science,90% of the world’s population is involved today in some form of religious or spiritual practice.1 Nonreligious people make up less than 0.1% of the populations in many Middle- Eastern and African countries. Only 8 of 238 countries have populations where more than 25% say they are not religious, and those are countries where the state has placed limitations on religious freedom. Atheism is actually rare around the world. More than 30 countries report no atheists (0%) and in only 12 of 238 countries do atheists make up 5% or more of the population. In Canada, 12.5% of the population are non- religious and 1.9% atheist. Evidence for religion playing a role in human life dates back 500 000 years ago when ritual treatment of skulls took place during China’s paleolithic period.2 Why has religion endured over this vast span of human history? What purpose has it served and does it continue to serve? I will argue that religion is a powerful coping behaviour that enables people to make sense of suffering, provides control over the overwhelming forces of nature (both internal and external), and promotes social rules that facilitate communal living, cooperation, and mutual support. Until recent times, religion and mental health care were closely aligned.3 Many of the first mental hospitals were
- 61. The Canadian Journal of Psychiatry, Vol 54, No 5, May 2009 � 283 Religious and spiritual factors are increasingly being examined in psychiatric research. Religious beliefs and practices have long been linked to hysteria, neurosis, and psychotic delusions. However, recent studies have identified another side of religion that may serve as a psychological and social resource for coping with stress. After defining the terms religion and spirituality, this paper reviews research on the relation between religion and (or) spirituality, and mental health, focusing on depression, suicide, anxiety, psychosis, and substance abuse. The results of an earlier systematic review are discussed, and more recent studies in the United States, Canada, Europe, and other countries are described. While religious beliefs and practices can represent powerful sources of comfort, hope, and meaning, they are often intricately entangled with neurotic and psychotic disorders, sometimes making it difficult to determine whether they are a resource or a liability. Can J Psychiatry. 2009;54(5):283–291. Clinical Implications � Religious beliefs and practices may be important resources for coping with illness. � Religious beliefs may contribute to mental pathology in some cases.
- 62. � Psychiatrists should be aware of patients’ religious and spiritual beliefs and seek to understand what function they serve. Limitations � My review of recent studies is selective, not systematic. � Studies without statistically significant findings are not discussed. � Clinical applications are not addressed. located in monasteries and run by priests. With some excep- tions, these religious institutions often treated patients with far more compassion than state-run facilities prior to 19th- century mental health reforms (reforms often led by religious people such as Dorothea Dix and William Tuke). In fact, the first form of psychiatric care in the United States was moral treatment, which involved the compassionate and humane treatment of people with mental illness—a revolutionary notion at a time when patients were often put on display and (or) housed in despicable conditions in the back wards of hos- pitals or prisons.4 Religion was believed to have a positive, civilizing influence on these patients, who might be rewarded for good conduct by allowing them to attend chapel services. However, in the late 19th century, the famous neurologist Jean Charcot and his star pupil, Sigmund Freud, began to associate religion with hysteria and neurosis. This created a deep divide that would separate religion from mental health care for the next century, as demonstrated by the writings of 3 generations of mental health professionals from Europe, the
- 63. United States, and Canada.5–8 Today, attitudes toward religion in psychiatry have begun to change. The American College of Graduate Medical Educa- tion now states in its Special Requirements for Residency Training for Psychiatry9 that all programs must provide train- ing on religious or spiritual factors that influence psychologi- cal development. Part of this change has been driven by scientific research during the past 2 decades that suggests reli- gious influences need not always be pathological, but can actually represent resources for health and well-being. Definitions Before reviewing the research, religion and spirituality must be defined, because these terms have ambiguous meanings that may affect the interpretation of research findings. The definition of religion is generally agreed on and involves beliefs, practices, and rituals related to the sacred. I define the sacred as that which relates to the numinous (mystical, super- natural) or God, and in Eastern religious traditions, to Ulti- mate Truth or Reality. Religion may also involve beliefs about spirits, angels, or demons. Religions usually have specific beliefs about life after death and rules about conduct that guide life within a social group. Religion is often organized and practiced within a community, but it can also be practiced alone and in private. However, central to its definition is that religion is rooted in an established tradition that arises out of a group of people with common beliefs and practices concern- ing the sacred. In contrast with religion, spirituality is more difficult to define. It is a more popular expression today than religion, as many view the latter as divisive and associated with war, con- flict, and fanaticism. Spirituality is considered more per- sonal, something people define for themselves that is largely
- 64. free of the rules, regulations, and responsibilities associated with religion. In fact, there is a growing group of people cate- gorized as spiritual-but-not-religious, who deny any connec- tion at all with religion and understand spirituality entirely in individualistic, secular terms. However, this contemporary use of spirituality is different from its original meaning. According to Philip Sheldrake,10 professor of applied theol- ogy at the University of Durham, England, the origin of the word spiritual lies in the Latin term spiritualis, which is derived from the Greek word pneumatikos, as it appears in Paul’s letters to the Romans and Corinthians. A spiritual per- son was considered someone with whom the Spirit of God dwelt, often referring to the clergy.10, p 3 In the Second Vatican Council, spirituality replaced terms such as ascetical theology and mystical theology. Although the Greeks used the word spiritual to distinguish humanity from nonrational creation, spiritual and (or) spirituality has been distinctly reli- gious throughout most of Western history. It was not until much later that Eastern religions adopted the term. Then, spiritual people were a subset of religious people whose lives and lifestyles reflected the teachings of their faith tradition. Spiritual people were those such as Teresa of Ávila, John of the Cross, Siddhartha Gautama, Mother Teresa, or Mahatma Gandhi. The term spirituality in health care has now expanded far beyond its original meaning. This expansion has resulted from attempts to be more inclusive in pluralistic health care settings, to address the needs both of religious and of non- religious people. This degree of inclusiveness, while admira- ble in the clinic, makes it impossible to conduct research on spirituality and relate it to mental health, as there is no unique, distinct, agreed-on definition. Thus researchers have strug- gled to come up with measures to assess spirituality.
- 65. When measured in research, spirituality is often assessed either in terms of religion or by positive psychological, social, or character states. For example, standard measures of spirituality today contain questions asking about meaning and purpose in life, connections with others, peacefulness, � La Revue canadienne de psychiatrie, vol 54, no 5, mai 2009284 In Review Abbreviations used in this article 5-HT 5-hydroxytryptamine (serotonin) 5-HT1A 5-beta hydroxytryptamine receptor 1 CASA National Center on Addiction and Substance Abuse MADRS Montgomery-Asberg Depression Rating Scale MDD major depressive disorder RCT randomized controlled trial RS religion and (or) spirituality existential well-being, and comfort and joy. This is problematic, as it assures that spirituality in such studies will be correlated with good mental health. In other words, spirituality—defined as good mental health and positive psychological or social traits—is found to correlate with good mental health. Such research is meaningless and tautological. To avoid this methodological problem and to maintain the
- 66. purity and distinctiveness of the construct, I have proposed that spirituality be defined in terms of religion,11 where reli- gion is a multidimensional construct not limited to institu- tional forms of religion. Thus I will either refer to religion or use the terms religion and spirituality synonymously (for example, as RS). Religion as a Coping Behaviour Systematic research in many countries around the world finds that religious coping is widespread. For the general popula- tion, research published in The New England Journal of Medi- cine found that 90% of Americans coped with the stress of September 11th (2001) by “turning to religion.”12, p 1507 During the week following the attacks, 60% of Americans attended a religious or memorial service and Bible sales rose 27%.13 Even prior to the year 2000, more than 60 studies had docu- mented high rates of religious coping in patients with an assortment of medical disorders ranging from arthritis to dia- betes to cancer.14 One systematic survey of hospitalized medi- cal patients (n = 330) found that 90% reported they used religion to cope, at least to a moderate extent, and more than 40% indicated that religion was the most important factor that kept them going.15 Psychiatric patients also frequently use religion to cope. A survey of patients (n = 406) with persistent mental illness at a Los Angeles County mental health facility found that more than 80% used religion to cope.16 In fact, most patients spent as much as one-half of their total coping time in religious prac- tices such as prayer. Researchers concluded that religion serves as a “pervasive and potentially effective method of coping for persons with mental illness, thus warranting its integration into psychiatric and psychological practice.”16, p
- 67. 660 In another study, conducted by the Center for Psychiatric Rehabilitation at Boston University, adults with severe mental illness were asked about the types of alternative health care practices they used.17 A total of 157 people with schizophre- nia, bipolar disorder, or MDD responded to the survey. People with schizophrenia and MDD reported that the most common beneficial alternative health practice was an RS activity (more than one-half reported this); for those with bipolar disorder, only meditation surpassed RS activity (54%, compared with 41%). Religious coping is likewise prevalent outside the United States. A study of psychiatric patients (n = 79) at Broken Hill Base Hospital in New South Wales found that 79% rated spir- ituality as very important, 82% thought their therapist should be aware of their spiritual beliefs and needs, and 67% indi- cated that spirituality helped them to cope with psychological pain.18 A survey of patients (n = 52) with lung cancer in Ontario asked about sources of emotional support. The most commonly reported support systems were family (79%) and religion (44%).19 Finally, a study of outpatients (n = 292) with cancer seen at the Northwestern Ontario Regional Can- cer Centre, Thunder Bay, found that, among all coping strate- gies inquired about, prayer was used by the highest number (64%).20 Why is religious coping so common among patients with medical and psychiatric illness? Religious beliefs provide a sense of meaning and purpose during difficult life circum- stances that assist with psychological integration; they usu- ally promote a positive world view that is optimistic and hopeful; they provide role models in sacred writings that facilitate acceptance of suffering; they give people a sense of
- 68. indirect control over circumstances, reducing the need for personal control; and they offer a community of support, both human and divine, to help reduce isolation and loneliness. Unlike many other coping resources, religion is available to anyone at any time, regardless of financial, social, physical, or mental circumstances. I will review studies examining the relation between religion and mental health in 5 areas: depression, suicide, anxiety, psychotic disorders, and substance abuse. While some stud- ies report no association between religious involvement and mental health, and a handful of studies have reported nega- tives associations, the majority (476 of 724 quantitative stud- ies prior to the year 2000, based on a systematic review) reported statistically significant positive associations.21 Because space is limited, I will briefly mention the results of that systematic review and then examine, in more detail, stud- ies that exemplify research published more recently. Depression Prior to 2000, more than 100 quantitative studies had exam- ined the relation between religion and depression.22 Among 93 observational studies, two-thirds found significantly lower rates of depressive disorder or fewer depressive symp- toms among the more religious. Among 34 studies that did not, only 4 found being religious was associated with signifi- cantly more depression. Among 22 longitudinal studies, 15 found that greater religiousness at baseline predicted fewer depression symptoms or faster remission of symptoms at follow-up. Among 8 RCTs, 5 found that religious-based psy- chological interventions resulted in faster symptom improve- ment, compared with secular-based therapy or with control subjects. Supporting these findings was a more recent
- 69. Research on Religion, Spirituality, and Mental Health: A Review The Canadian Journal of Psychiatry, Vol 54, No 5, May 2009 � 285 independently published meta-analysis of 147 studies that involved nearly 100 000 subjects.23 The average inverse cor- relation between religious involvement and depression was –0.10, which increased to –0.15 for studies in stressed popula- tions. While this correlation appears small and weak, it is of the same magnitude as seen for sex (a widely recognized fac- tor influencing the prevalence of depression). Moreover, individual studies in stressed populations, particu- larly people with serious medical illness, find a more substan- tial impact for religion on the prevalence and course of depression. For example, depressed medical inpatients (n = 1000) aged 50 years or older with either congestive heart fail- ure or chronic pulmonary disease were identified with depres- sive disorder using the Structured Clinical Interview for Depression.24 The religious characteristics of these patients were compared with those of nondepressed patients (n = 428). Depressed patients were significantly more likely to indicate no religious affiliation, more likely to indicate spiritual but not religious, less likely to pray or read scripture, and scored lower on intrinsic religiosity. These relations remained robust after controlling for demographic, social, and physical health factors. Among the depressed patients, severity of depressive symptoms was also inversely related to religious indicators. Among these 1000 depressed patients, investigators followed 865 for 12 to 24 weeks, examining factors influencing speed of remission from depression.25 The most religious patients
- 70. (those who attended religious services at least weekly, prayed at least daily, read the Bible or other religious scriptures at least 3 times weekly, and scored high on intrinsic religiosity) remitted from depression more than 50% faster than other patients (hazard ratio = 1.53, 95% CI 1.20 to 1.94), controlling for multiple demographic, psychosocial, psychiatric, and physical health predictors of remission. Several other studies have similarly shown a positive impact for religion on course of depression.26–28 However, for psychiatric patients there have been few studies on the course of depression. Bosworth et al29 interviewed elderly psychiatric inpatients (n = 104), assessing public and private religious practices and religious coping. Depressive symptoms were assessed at baseline and 6 months later by a psychiatrist using the MADRS. Baseline positive religious coping predicted significantly less depression on the MADRS at the 6-month evaluation, an effect independent of social sup- port measures, demographics, use of electroconvulsive ther- apy, and number of depressive episodes. At least 2 studies (both cross-sectional) have examined rela- tions between religious involvement and depression in Canada, one reporting an inverse relation and the other find- ing a positive relation. O’Connor and Vallerand30 examined associations between religious motivation and personal adjustment in a sample of elderly French-Canadians (n = 176) drawn from nursing homes in the greater Montreal area. Intrinsic religiosity was inversely related to depression and positively related to life satisfaction, self-esteem, and mean- ing in life. In the second study, Sorenson et al31 followed teenaged mothers (n = 261) (87% unmarried) before delivery and 4 weeks after delivery in southwestern Ontario. They examined the relation between religion and depressive symp- toms during the first few weeks after babies were born. Cath-
- 71. olics and teenagers affiliated with more conservative religious groups scored significantly higher on depression, and those who attended religious services more frequently also had higher depression scores. However, the highest depression scores were among girls who cohabitated with someone while continuing to attend religious services. Baetz and colleagues32,33 have shown in large cross-sectional community surveys of the Canadian population that religious attendance is associated with less depression and fewer psy- chiatric disorders. However, participants indicating that spir- itual values were important or perceived themselves as spiritual or religious had higher levels of psychiatric symp- toms. The researchers speculated that these people could have turned to RS to reframe difficult life circumstances associated with psychiatric illness. Bear in mind that the stud- ies were conducted in largely healthy community-dwelling adults with relatively low stress levels. Two additional unpublished dissertations34,35 report studies of RS and depression in Canadian men with prostate cancer and in bereaved caregivers of Canadians dying from AIDS. Both demonstrated positive effects for RS involvement on posttraumatic growth and coping with illness. Supporting the findings of the Canadian caregiver study, Fenix et al36 at Yale University recently followed caregivers (n = 175) of recently deceased cancer patients for 13 months, examining associa- tions between religiousness and the development of MDD.36 Religious caregivers were significantly less likely to have developed MDD by the 13-month follow-up, a finding that persisted after adjusting for other risk factors. The same results have been reported for caregivers of patients with Alzheimer disease.37,38 Thus studies in medical patients, older adults with serious
- 72. and disabling medical conditions, and their caregivers sug- gest that religious involvement is an important factor that enables such people to cope with stressful health problems and life circumstances. However, this may not be true in all populations, as studies of pregnant unmarried teenagers and nonstressed community populations above suggest. Critics say that most studies reporting positive results are observational and that some unmeasured characteristic may be related both to religion and to depression, confounding the � La Revue canadienne de psychiatrie, vol 54, no 5, mai 2009286 In Review relation. In particular, genetic factors have been implicated. In a fascinating study that examined the relation of spirituality to brain 5-HT1A binding using positive emission tomography, investigators found that 5-HT1A binding was lower in people who were more spiritually accepting. Note that lower 5-HT1A binding—the same pattern seen with spirituality—has been found in patients with anxiety and depressive disorders.39–41 Thus, rather than being genetically less prone to depression, RS-oriented people may be at increased risk for mood disorders based on their 5-HT receptor binding profile. Suicide In Koenig et al’s42 systematic review of research conducted before 2000, 68 studies were identified that examined the religion–suicide relation. Among those studies, 57 found fewer suicides or more negative attitudes toward suicide
- 73. among the more religious, 9 showed no relation, and 2 reported mixed results. Seven of the studies were conducted in Canada, and of those, 5 found fewer suicides or more negative attitudes toward suicide among the more religious, 1 found no association, and 1 reported mixed results. While recent research suggests that religion prevents suicide primarily through religious doctrines that prohibit suicide,43 there is also evidence that the comfort and meaning derived from religious beliefs may be relevant44 and may be especially important in people with advanced medical illness.45 Reli- gious involvement may also help to prevent suicide by sur- rounding the person at risk with a caring, supportive community.46 Anxiety While religious teachings have the potential to exacerbate guilt and fear that reduce quality of life or otherwise interfere with functioning, the anxiety aroused by religious beliefs can prevent behaviours harmful to others and motivate pro-social behaviours. Religious beliefs and practices can also comfort people who are fearful or anxious, increase sense of control, enhance feelings of security, and boost self-confidence (or confidence in Divine beings). Prior to 2000, at least 76 studies had examined the relation between religious involvement and anxiety.47 Sixty-nine studies were observational and 7 were RCTs. Among the observational studies, 35 found significantly less anxiety or fear among the more religious, 24 found no association, and 10 reported greater anxiety. However, all 10 of the latter stud- ies were cross-sectional, and anxiety and (or) fear is a strong motivator of religious activity. People pray more when they are scared or nervous and feel out of control (“There are no
- 74. atheists in foxholes”). Then, cross-sectional studies are less useful than longitudinal studies or RCTs. Among the 7 RCTs examining the effects of a religious intervention on subjects with anxiety (usually generalized anxiety disorder), 6 found that religious interventions in religious patients reduced anx- iety levels more quickly than secular interventions or control subjects. Studies of Eastern spiritual techniques, such as mindfulness meditation (from the Buddhist tradition), report similar effects,48,49 although their efficacy in anxiety disor- ders has recently been questioned.50 More recent longitudinal studies add to this literature, and provide information on mechanisms. Wink and Scott51 fol- lowed subjects (n = 155) for nearly 30 years, from middle age into later life, studying the impact of religious beliefs and involvement on death anxiety. Analyses revealed no linear relations between religiousness, fear of death, and fear of dying. Subjects with the lowest anxiety levels were those who were either high or low on religiousness. Anxiety was highest among subjects who were only moderately religious, and in particular, those who affirmed belief in an afterlife but were not involved in any religious practices. Researchers concluded that it was the degree of religious involvement that was important in lessening death anxiety not simply belief in an afterlife. Religious involvement may also interact with certain forms of psychotherapy to enhance response to therapy. Investiga- tors at the University of Saskatchewan explored coping and motivation factors related to treatment response in patients (n = 56) with panic disorder participating in a clinical trial.52 Subjects were treated with group cognitive-behavioural ther- apy, and then were followed up at 6 and 12 months after base- line evaluation. Self-rated importance of religion was a